

Association Between Plasma Caffeine and Other Methylxanthines and Metabolic Parameters in a Psychiatric Population Treated With Psychotropic Drugs Inducing Metabolic Disturbances
- PMID: 30473668
- PMCID: PMC6238296
- DOI: 10.3389/fpsyt.2018.00573
Association Between Plasma Caffeine and Other Methylxanthines and Metabolic Parameters in a Psychiatric Population Treated With Psychotropic Drugs Inducing Metabolic Disturbances
Abstract
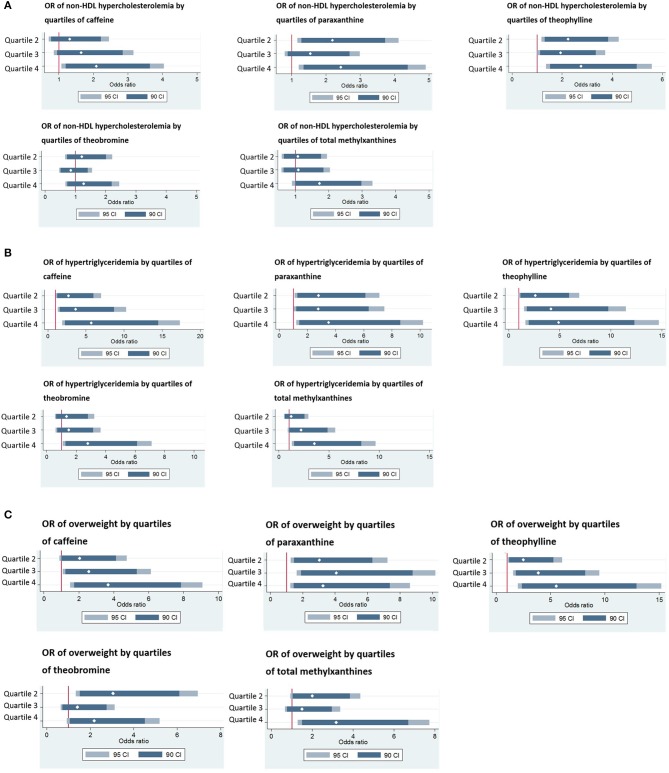
Importance: Multiple studies conducted in the general population identified an association between self-reported coffee consumption and plasma lipid levels. To date, no study assessed whether and which plasma methylxanthines (caffeine and/or its metabolites, i.e., paraxanthine, theophylline, and theobromine) are associated with plasma lipids. In psychiatric patients, an important coffee consumption is often reported and many psychotropic drugs can induce a rapid and substantial increase of plasma lipid levels. Objective: To determine whether plasma methylxanthines are associated with metabolic parameters in psychiatric patients receiving treatments known to induce metabolic disturbances. Design, Setting, and Participants: Data were obtained from a prospective study including 630 patients with metabolic parameters [i.e., body mass index (BMI), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), non-high-density lipoprotein cholesterol (non-HDL-C), and fasting triglycerides (TG)] monitored routinely during psychotropic treatment. Exposures: Plasma methylxanthines levels. Main Outcomes and Measures: Metabolic variables including BMI and plasma lipid levels. Results: Multivariate analyses indicated that BMI, TC, HDL-C, and non-HDL-C increased significantly with increasing total methylxanthines (p corrected ≤ 0.05). In addition, compared to patients with plasma caffeine concentration in the lowest quartile, those with caffeine concentration in the highest quartile were twice more prone to suffer from non-HDL hypercholesterolemia (p corrected = 0.05), five times more likely to suffer from hypertriglyceridemia (p corrected = 0.01) and four times more susceptible to be overweight (p corrected = 0.01). Conclusions and Relevance: This study showed that plasma caffeine and other methylxanthines are associated with worsening of metabolic parameters in patients receiving psychotropic treatments known to induce metabolic disturbances. It emphasizes that important caffeine consumption could be considered as an additional environmental risk factor for metabolic worsening in patients receiving such treatments.
Keywords: lipids; metabolic parameters; plasma caffeine level; plasma methylxanthines; psychotropic drugs; secondary effects.
Figures
Similar articles
-
Associations Between High Plasma Methylxanthine Levels, Sleep Disorders and Polygenic Risk Scores of Caffeine Consumption or Sleep Duration in a Swiss Psychiatric Cohort.Front Psychiatry. 2021 Dec 20;12:756403. doi: 10.3389/fpsyt.2021.756403. eCollection 2021. Front Psychiatry. 2021. PMID: 34987426 Free PMC article.
-
Investigating the Relations Between Caffeine-Derived Metabolites and Plasma Lipids in 2 Population-Based Studies.Mayo Clin Proc. 2021 Dec;96(12):3071-3085. doi: 10.1016/j.mayocp.2021.05.030. Epub 2021 Sep 25. Mayo Clin Proc. 2021. PMID: 34579945
-
Early changes of blood lipid levels during psychotropic drug treatment as predictors of long-term lipid changes and of new onset dyslipidemia.J Clin Lipidol. 2018 Jan-Feb;12(1):219-229. doi: 10.1016/j.jacl.2017.10.002. Epub 2017 Oct 16. J Clin Lipidol. 2018. PMID: 29128242
-
The toxicology of cocoa and methylxanthines: a review of the literature.Crit Rev Toxicol. 1982;9(4):275-312. doi: 10.3109/10408448209037495. Crit Rev Toxicol. 1982. PMID: 6765610 Review.
-
Methylxanthines: toxicity to humans. 3. Theobromine, paraxanthine and the combined effects of methylxanthines.Food Chem Toxicol. 1988 Aug;26(8):725-33. doi: 10.1016/0278-6915(88)90073-7. Food Chem Toxicol. 1988. PMID: 3058562 Review.
Cited by
-
Social dynamics modeling of chrono-nutrition.PLoS Comput Biol. 2019 Jan 30;15(1):e1006714. doi: 10.1371/journal.pcbi.1006714. eCollection 2019 Jan. PLoS Comput Biol. 2019. PMID: 30699206 Free PMC article.
-
Self-reported caffeine consumption miss-matched consumption measured by plasma levels of caffeine and its metabolites: results from two population-based studies.Eur J Nutr. 2024 Aug;63(5):1555-1564. doi: 10.1007/s00394-024-03351-9. Epub 2024 May 4. Eur J Nutr. 2024. PMID: 38703227 Free PMC article.
-
Associations Between High Plasma Methylxanthine Levels, Sleep Disorders and Polygenic Risk Scores of Caffeine Consumption or Sleep Duration in a Swiss Psychiatric Cohort.Front Psychiatry. 2021 Dec 20;12:756403. doi: 10.3389/fpsyt.2021.756403. eCollection 2021. Front Psychiatry. 2021. PMID: 34987426 Free PMC article.
References
-
- Burr ML, Limb ES, Sweetnam PM, Fehily AM, Amarah L, Hutchings A. Instant coffee and cholesterol: a randomised controlled trial. Eur J Clin Nutr. (1995) 49:779–84. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous