

Recent advances in imaging and understanding interstitial cystitis
- PMID: 30473772
- PMCID: PMC6234747
- DOI: 10.12688/f1000research.16096.1
Recent advances in imaging and understanding interstitial cystitis
Abstract
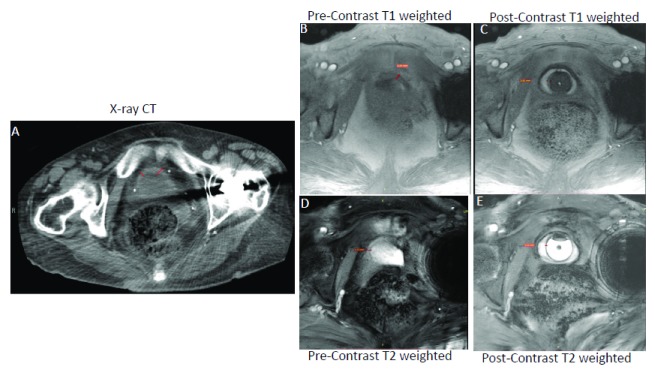
Interstitial cystitis/bladder pain syndrome (IC/BPS) is a debilitating condition associated with intense pelvic pain and bladder storage symptoms. Since diagnosis is difficult, prevalence estimates vary with the methodology used. There is also a lack of proven imaging tools and biomarkers to assist in differentiation of IC/BPS from other urinary disorders (overactive bladder, vulvodynia, endometriosis, and prostatitis). Current uncertainty regarding the etiology and pathology of IC/BPS ultimately impacts its timely and successful treatment, as well as hampers future drug development. This review will cover recent developments in imaging methods, such as magnetic resonance imaging, that advance the understanding of IC/BPS and guide drug development.
Keywords: Interstitial cystitis; MRI; bladder wall; fibrosis; imaging; radiation.
Conflict of interest statement
Competing interests: Joseph Janicki is an employee of Lipella Pharmaceuticals, whereas Jonathan Kaufman and Michael Chancellor are inventors of novel contrast mixture. Pradeep Tyagi, Chan-Hong Moon, Naoki Yoshimura and Christopher Chermansky declare that they have no competing interests.No competing interests were disclosed.No competing interests were disclosed.
Figures
References
-
- Suskind AM, Berry SH, Ewing BA, et al. : The prevalence and overlap of interstitial cystitis/bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: results of the RAND Interstitial Cystitis Epidemiology male study. J Urol. 2013;189(1):141–5. 10.1016/j.juro.2012.08.088 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical