

Endovascular Fenestration/Stenting First Followed by Delayed Open Aortic Repair for Acute Type A Aortic Dissection With Malperfusion Syndrome
- PMID: 30474418
- PMCID: PMC6339462
- DOI: 10.1161/CIRCULATIONAHA.118.036328
Endovascular Fenestration/Stenting First Followed by Delayed Open Aortic Repair for Acute Type A Aortic Dissection With Malperfusion Syndrome
Abstract
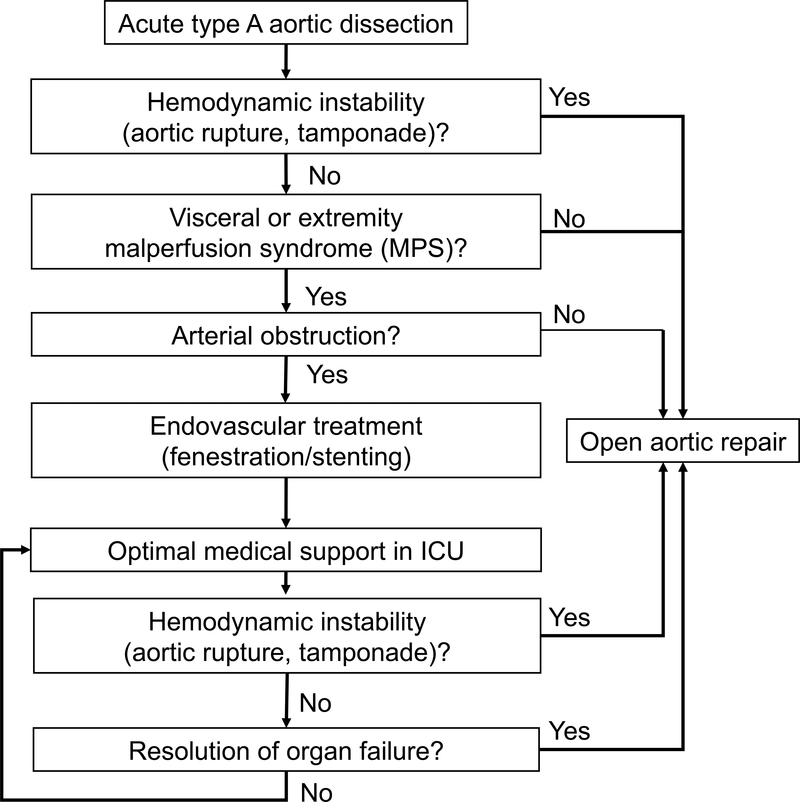
Background: Immediate open repair of acute type A aortic dissection is traditionally recommended to prevent death from aortic rupture. However, organ failure because of malperfusion syndrome (MPS) might be the most imminent life-threatening problem for a subset of patients.
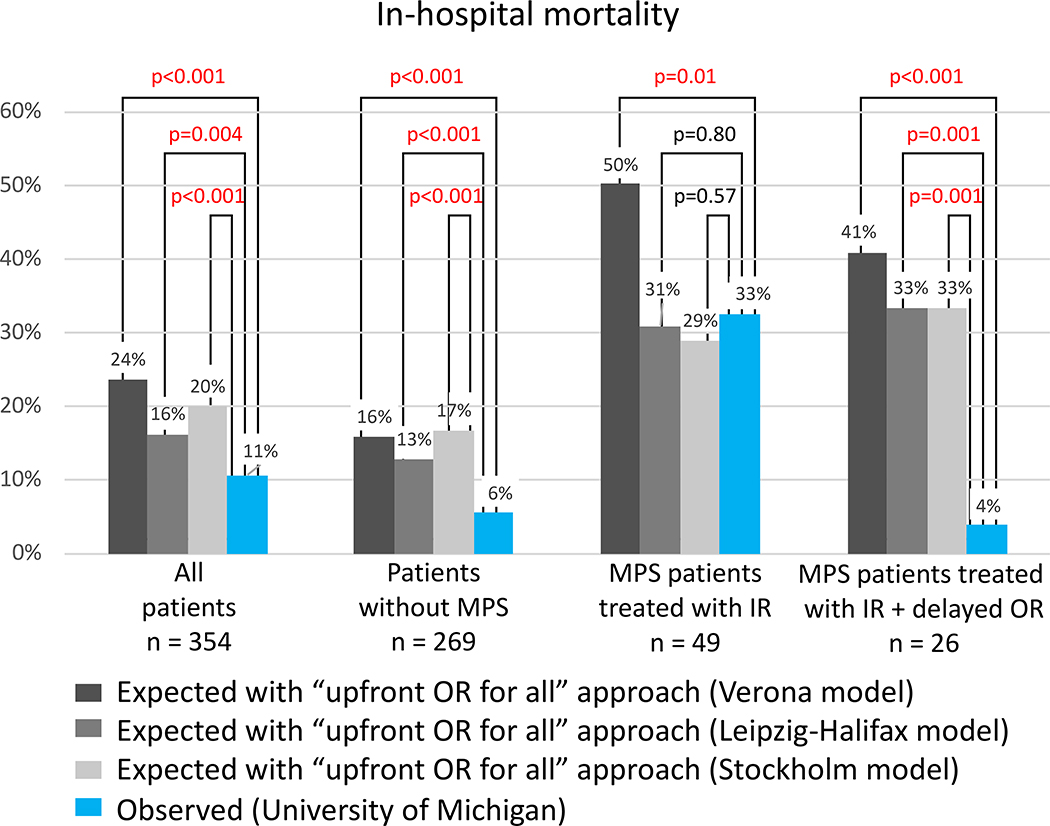
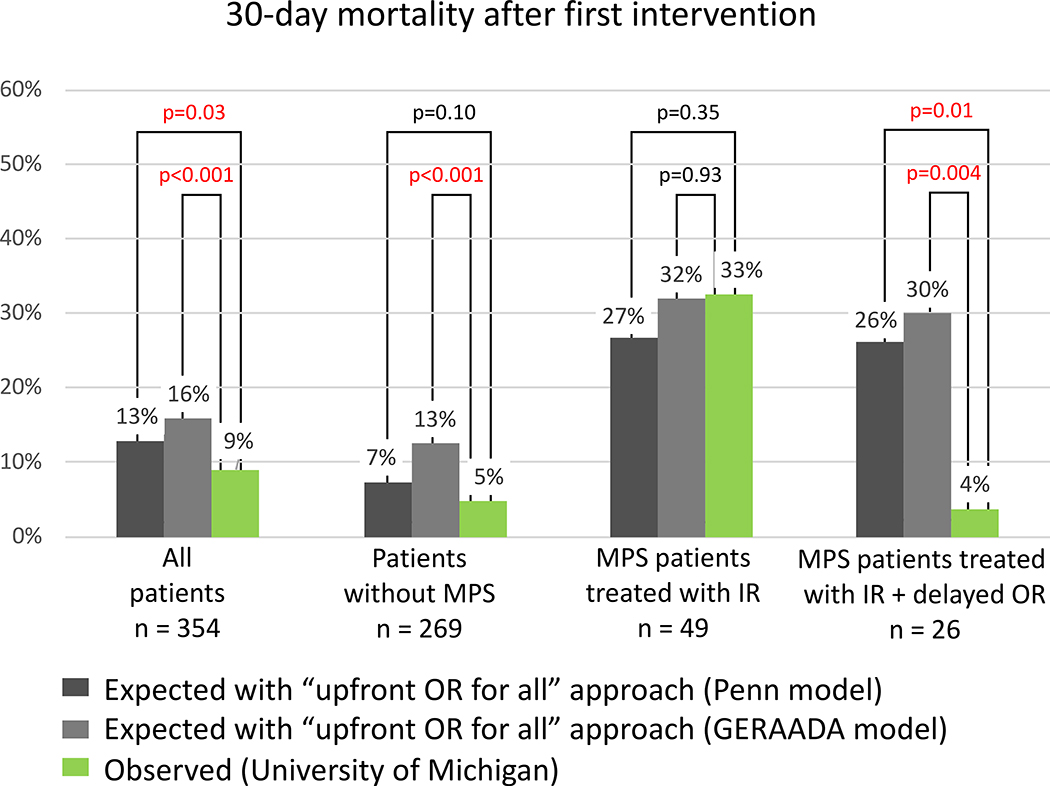
Methods: From 1996 to 2017, among 597 patients with acute type A aortic dissection, 135 patients with MPS were treated with upfront endovascular reperfusion (fenestration/stenting) followed by delayed open repair (OR). We compared outcomes between the first and second decades and observed mortalities with those expected with an "upfront OR for every patient" approach, determined using prognostic models from the literature (Verona, Leipzig-Halifax, Stockholm, Penn, and GERAADA [German Registry for Acute Aortic Dissection Type A] models).
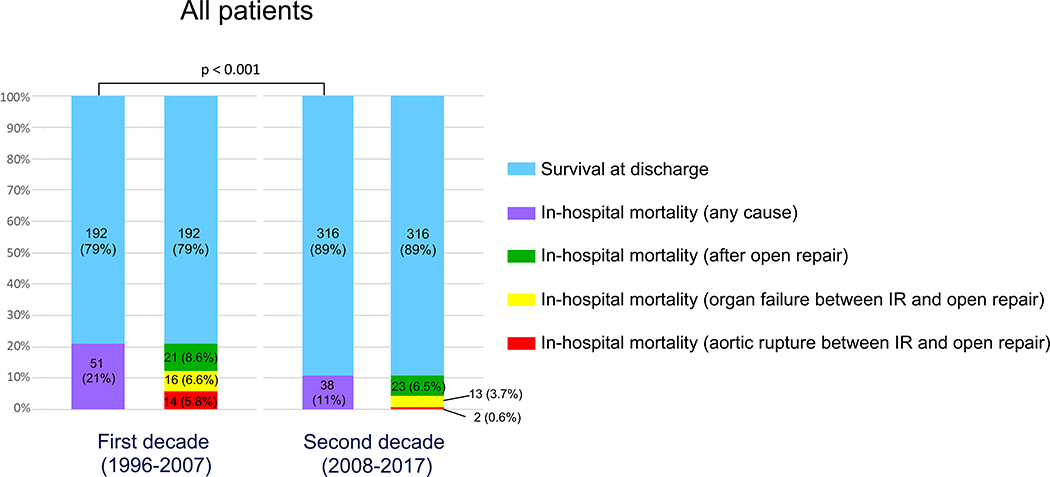
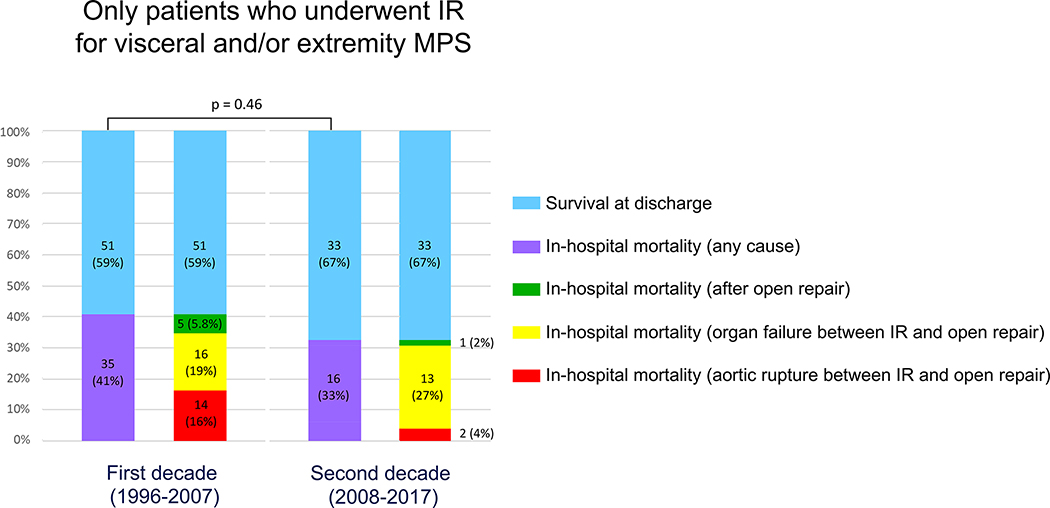
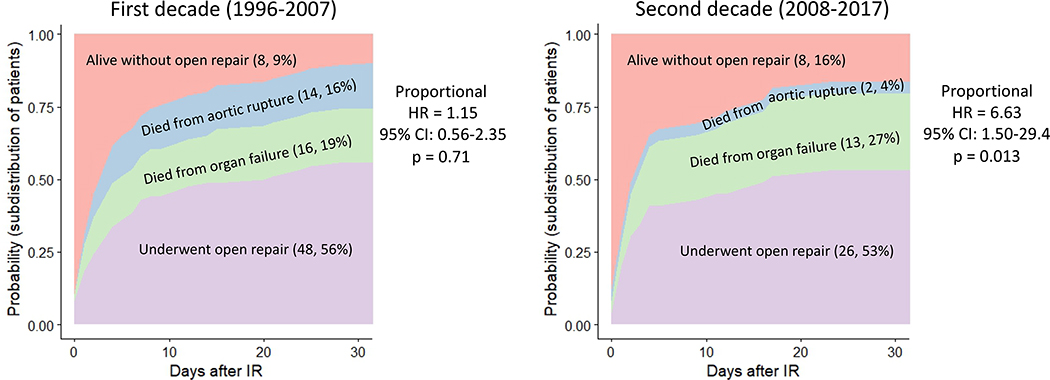
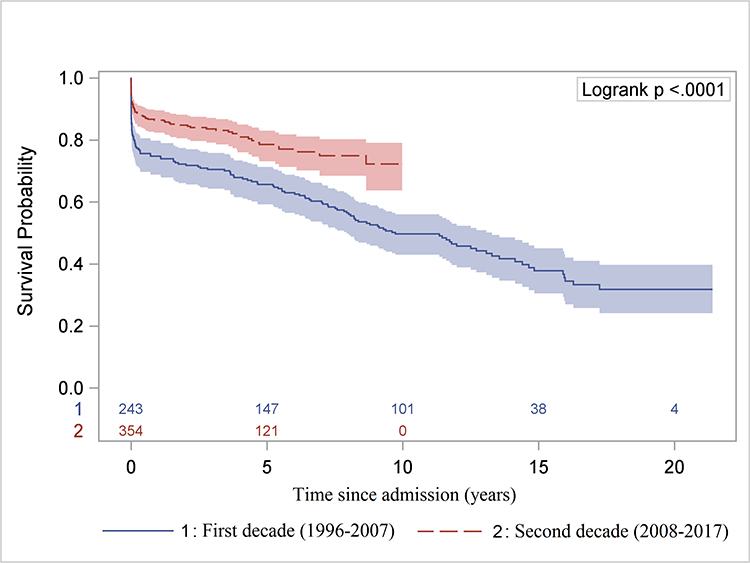
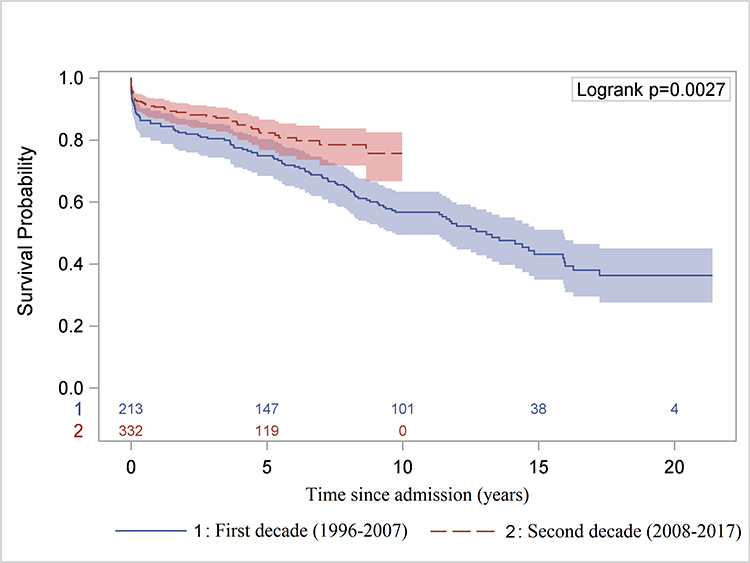
Results: Overall, in-hospital mortality improved between the 2 decades (21.0% versus 10.7%, P<0.001). In the second decade, for patients with MPS initially treated with fenestration/stenting, mortality from aortic rupture decreased from 16% to 4% ( P=0.05), the risk of dying from organ failure was 6.6 times higher than dying from aortic rupture (hazard ratio=6.63; 95% CI, 1.5-29; P=0.01), and 30-day mortality after OR for MPS patients was 3.7%. Compared to the expected mortalities with the upfront OR for every patient models, our observed 30-day and in-hospital mortalities (9% and 11%, respectively) of all patients with acute type A aortic dissection were significantly lower ( P≤0.03).
Conclusions: Immediate OR is the strategy to prevent death from aortic rupture for the majority of patients with acute type A aortic dissection. However, relatively stable (no rupture, no tamponade) patients with MPS benefit from a staged approach: upfront endovascular reperfusion followed by aortic OR at resolution of organ failure.
Keywords: acute aortic syndrome; acute cardiac care; aortic disease; aortic dissection; aortic surgery; endovascular fenestration/stenting; malperfusion; malperfusion syndrome.
Conflict of interest statement
DISCLOSURES:
No conflicts of interest related to this study to disclose.
Figures
Comment in
-
Upfront Interventional Radiology for Acute Type A Dissection With Malperfusion Syndrome.Circulation. 2018 Nov 6;138(19):2104-2105. doi: 10.1161/CIRCULATIONAHA.118.037858. Circulation. 2018. PMID: 30474421 No abstract available.
References
-
- Toda R, Moriyama Y, Masuda H, Iguro Y, Yamaoka A, Taira A. Organ malperfusion in acute aortic dissection. Jpn J Thorac Cardiovasc Surg. 2000;48:545–550. - PubMed
-
- Mehta RH, Suzuki T, Hagan PG, Bossone E, Gilon D, Llovet A, Maroto LC, Cooper JV, Smith DE, Armstrong WF, Nienaber CA, Eagle KA; International Registry of Acute Aortic Dissection (IRAD) Investigators. Predicting death in patients with acute type A aortic dissection. Circulation. 2002;105:200–206. - PubMed
-
- Girardi LN, Krieger KH, Lee LY, Mack CA, Tortolani AJ, Isom OW. Management strategies for type A dissection complicated by peripheral vascular malperfusion. Ann Thorac Surg. 2004;77:1309–1314; discussion 1314. - PubMed
-
- Trimarchi S, Nienaber CA, Rampoldi V, Myrmel T, Suzuki T, Mehta RH, Bossone E, Cooper JV, Smith DE, Menicanti L, Frigiola A, Oh JK, Deeb MG, Isselbacher EM, Eagle KA, International Registry of Acute Aortic Dissection Investigators. Contemporary results of surgery in acute type A aortic dissection: the International Registry of Acute Aortic Dissection experience. J Thorac Cardiovasc Surg. 2005:129:112–122. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
