

Rapid Self-Assembly of Bioengineered Cardiovascular Bypass Grafts From Scaffold-Stabilized, Tubular Bilevel Cell Sheets
- PMID: 30474423
- PMCID: PMC6261325
- DOI: 10.1161/CIRCULATIONAHA.118.035231
Rapid Self-Assembly of Bioengineered Cardiovascular Bypass Grafts From Scaffold-Stabilized, Tubular Bilevel Cell Sheets
Abstract
Background: Cardiovascular bypass grafting is an essential treatment for complex cases of atherosclerotic disease. Because the availability of autologous arterial and venous conduits is patient-limited, self-assembled cell-only grafts have been developed to serve as functional conduits with off-the-shelf availability. The unacceptably long production time required to generate these conduits, however, currently limits their clinical utility. Here, we introduce a novel technique to significantly accelerate the production process of self-assembled engineered vascular conduits.
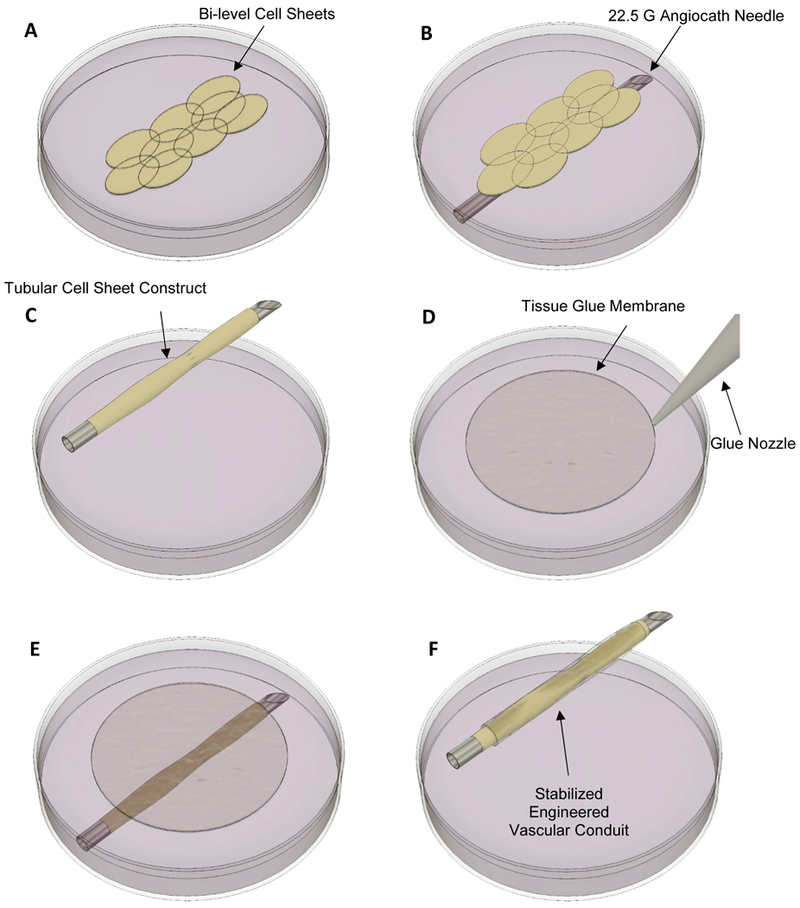
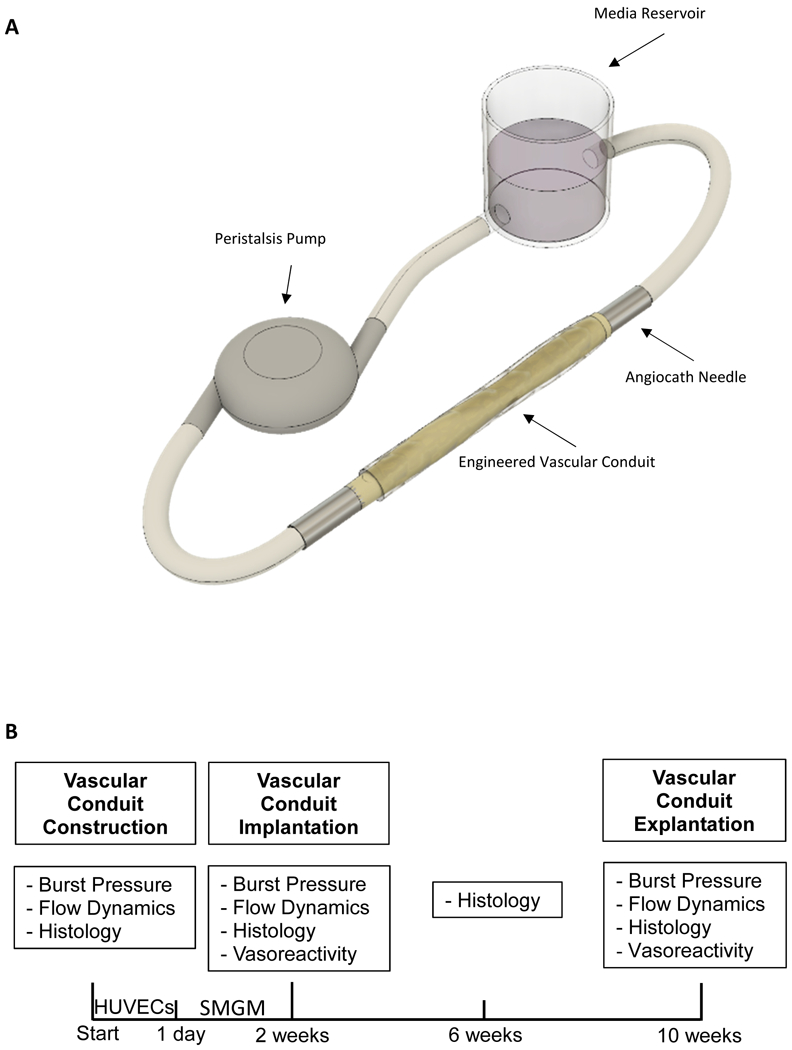
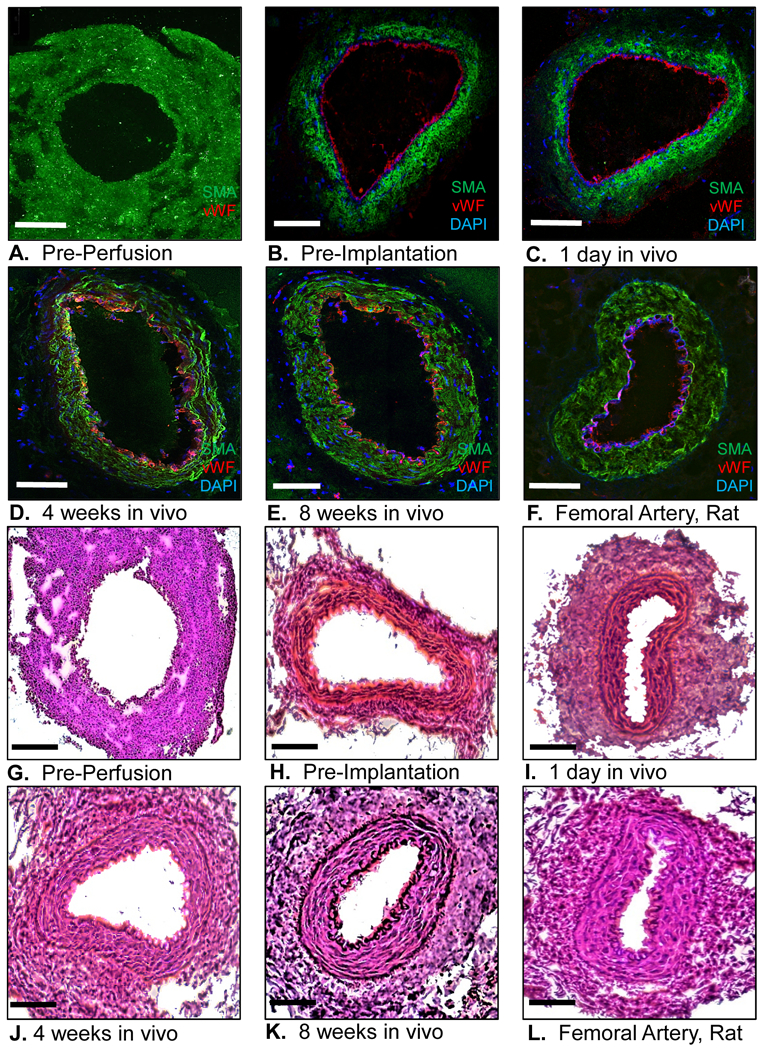
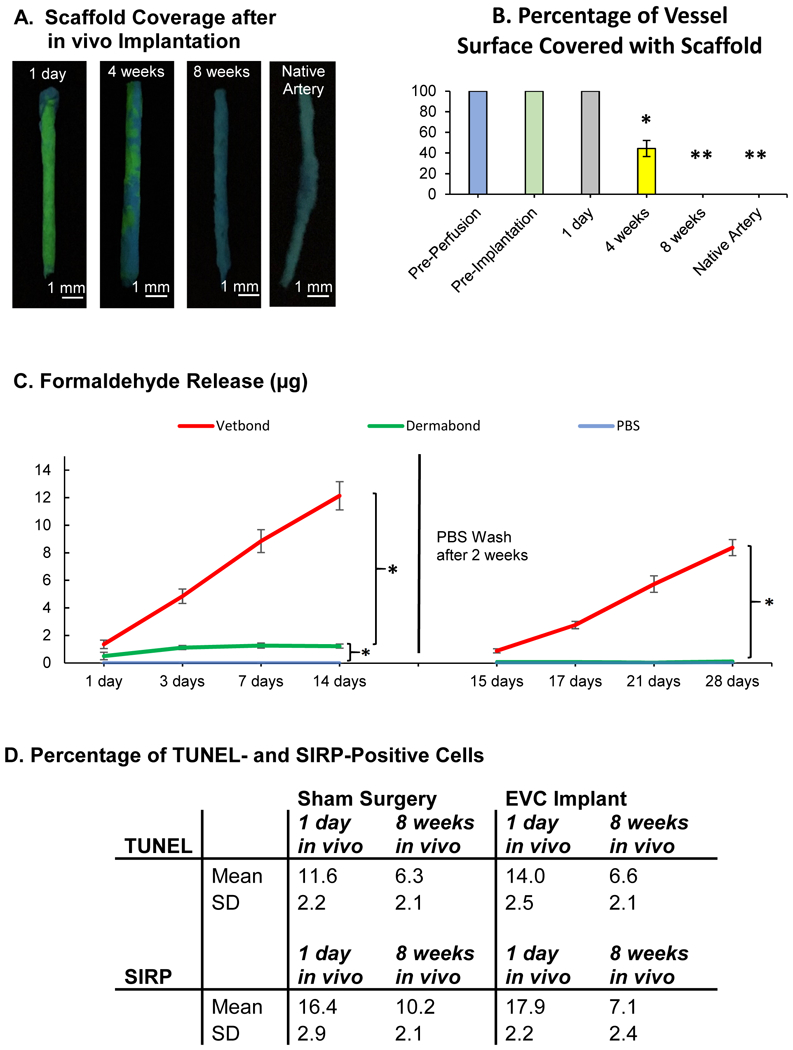
Methods: Human aortic smooth muscle cells and skin fibroblasts were used to construct bilevel cell sheets. Cell sheets were wrapped around a 22.5-gauge Angiocath needle to form tubular vessel constructs. A thin, flexible membrane of clinically approved biodegradable tissue glue (Dermabond Advanced) served as a temporary, external scaffold, allowing immediate perfusion and endothelialization of the vessel construct in a bioreactor. Subsequently, the matured vascular conduits were used as femoral artery interposition grafts in rats (n=20). Burst pressure, vasoreactivity, flow dynamics, perfusion, graft patency, and histological structure were assessed.
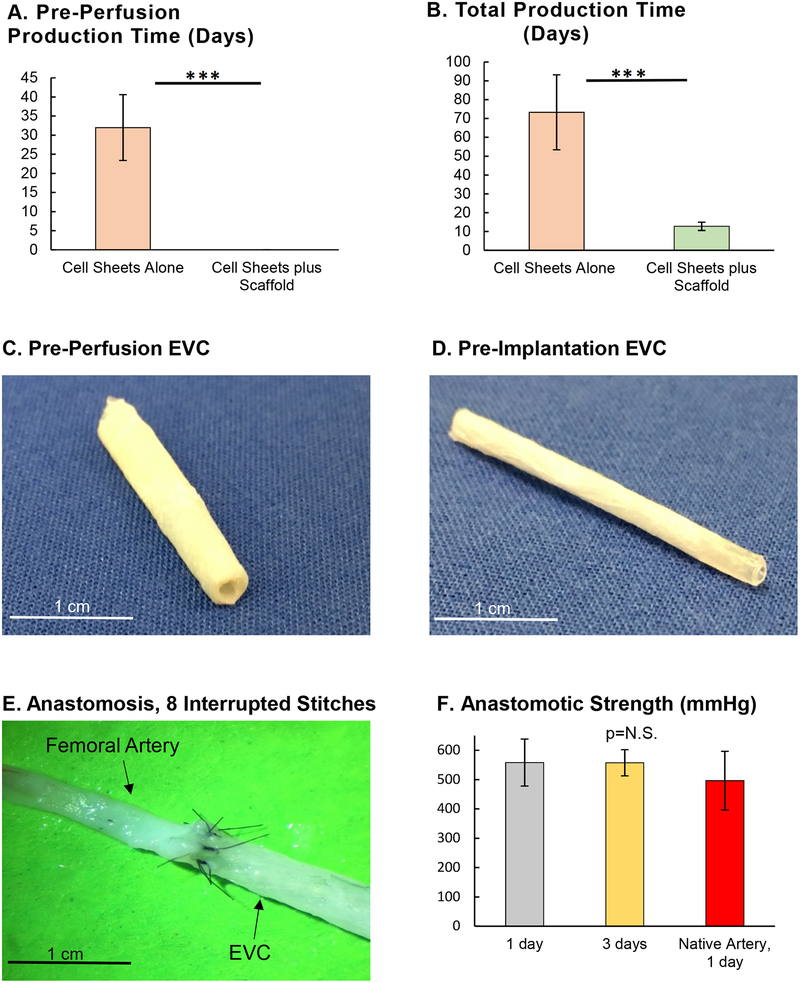
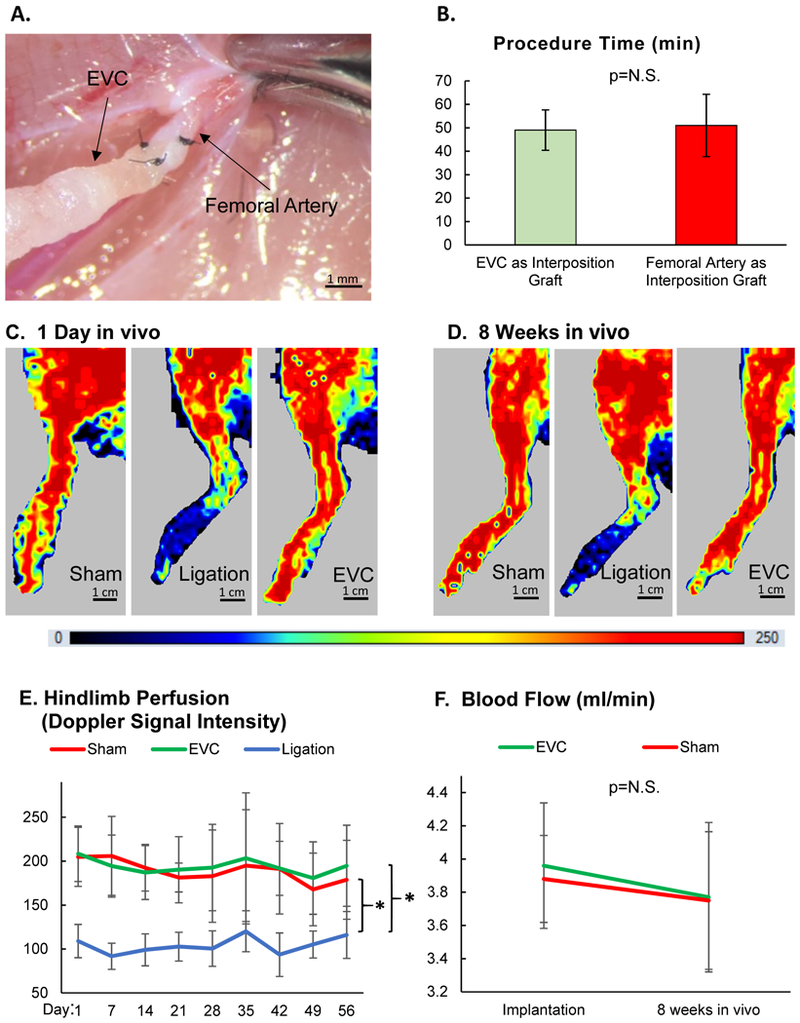
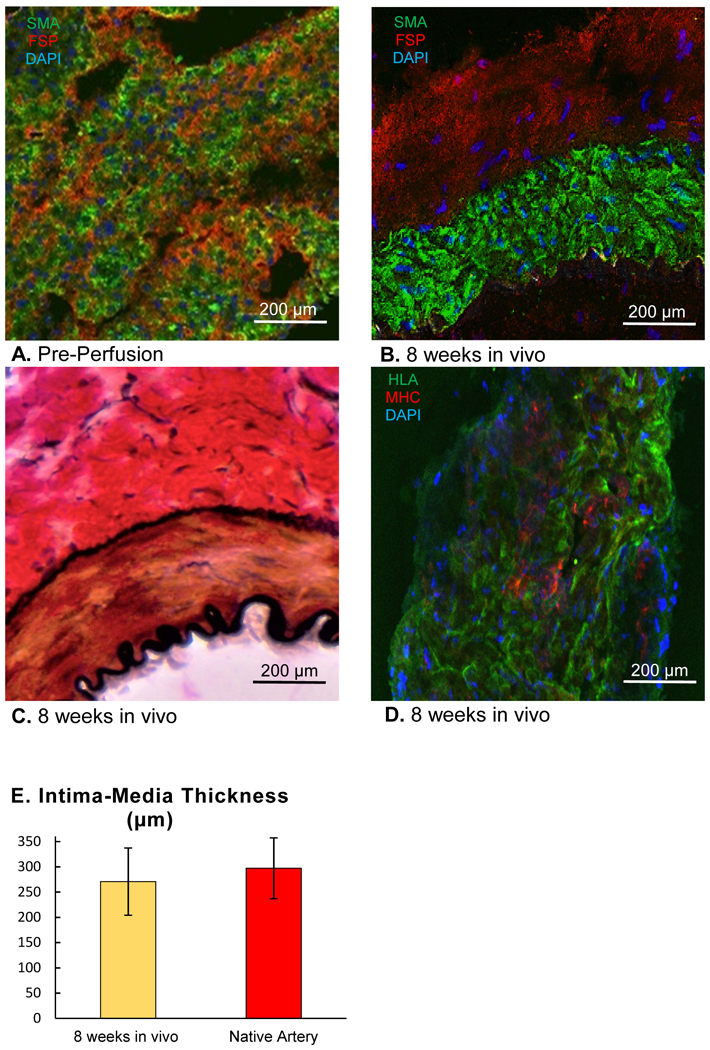
Results: Compared with engineered vascular conduits formed without external stabilization, glue membrane-stabilized conduits reached maturity in the bioreactor in one-fifth the time. After only 2 weeks of perfusion, the matured conduits exhibited flow dynamics similar to that of control arteries, as well as physiological responses to vasoconstricting and vasodilating drugs. The matured conduits had burst pressures exceeding 500 mm Hg and had sufficient mechanical stability for surgical anastomoses. The patency rate of implanted conduits at 8 weeks was 100%, with flow rate and hind-limb perfusion similar to those of sham controls. Grafts explanted after 8 weeks showed a histological structure resembling that of typical arteries, including intima, media, adventitia, and internal and external elastic membrane layers.
Conclusions: Our technique reduces the production time of self-assembled, cell sheet-derived engineered vascular conduits to 2 weeks, thereby permitting their use as bypass grafts within the clinical time window for elective cardiovascular surgery. Furthermore, our method uses only clinically approved materials and can be adapted to various cell sources, simplifying the path toward future clinical translation.
Keywords: bioengineering; bioreactors; coronary artery bypass; tissue adhesive; vascular grafting.
Figures

References
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, de Ferranti SD, Ferguson JF, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Lutsey PL, Mackey JS, Matchar DB, Matsushita K, Mussolino ME, Nasir K, O’Flaherty M, Palaniappan LP, Pandey A, Pandey DK, Reeves MJ, Ritchey MD, Rodriguez CJ, Roth GA, Rosamond WD, Sampson UKA, Satou GM, Shah SH, Spartano NL, Tirschwell DL, Tsao CW, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018;137:e67–e492. - PubMed
-
- Eagle KA, Guyton RA, Davidoff R, Edwards FH, Ewy GA, Gardner TJ, Hart JC, Herrmann HC, Hillis LD, Hutter AM, Lytle BW, Marlow RA, Nugent WC, Orszulak TA, American College of Cardiology, American Heart Association. ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). Circulation. 2004;110:e340–437. - PubMed
-
- Alexander JH, Smith PK. Coronary-Artery Bypass Grafting. N Engl J Med. 2016;374:1954–1964. - PubMed
-
- Goldman S, Zadina K, Moritz T, Ovitt T, Sethi G, Copeland JG, Thottapurathu L, Krasnicka B, Ellis N, Anderson RJ, Henderson W, VA Cooperative Study Group #207/297/364. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: results from a Department of Veterans Affairs Cooperative Study. J Am Coll Cardiol. 2004;44:2149–2156. - PubMed
-
- Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR. Coronary bypass graft fate and patient outcome: angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years. J Am Coll Cardiol. 1996;28:616–626. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
