

Chylothorax after hepatectomy: a case report
- PMID: 30474568
- PMCID: PMC6260677
- DOI: 10.1186/s13256-018-1882-x
Chylothorax after hepatectomy: a case report
Abstract
Background: Chylothorax is the accumulation of chyle within the pleural space. Chylothorax can occur as a complication after multiple different types of surgery, most frequently after thoracic surgery, albeit with an incidence rate of less than 1%. Chylothorax after abdominal surgery is extremely rare, and there are only a few case reports.
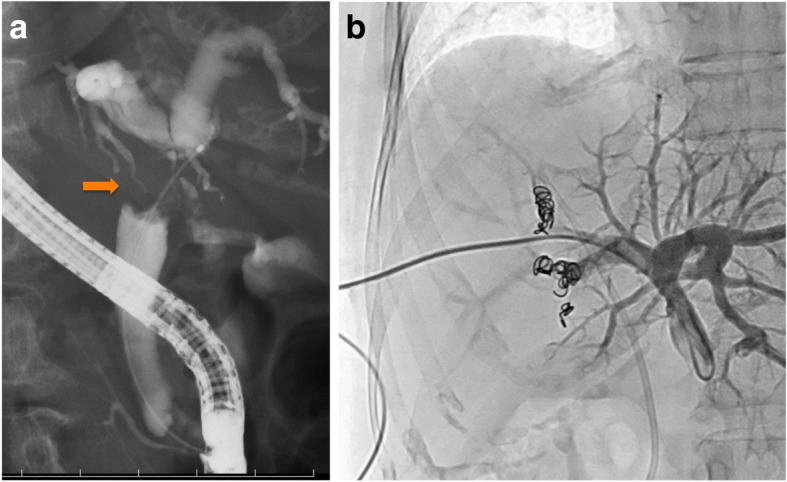
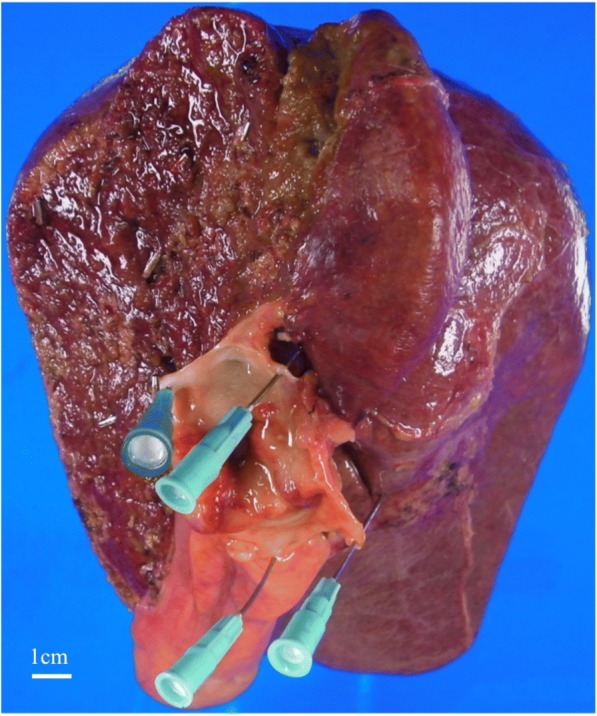
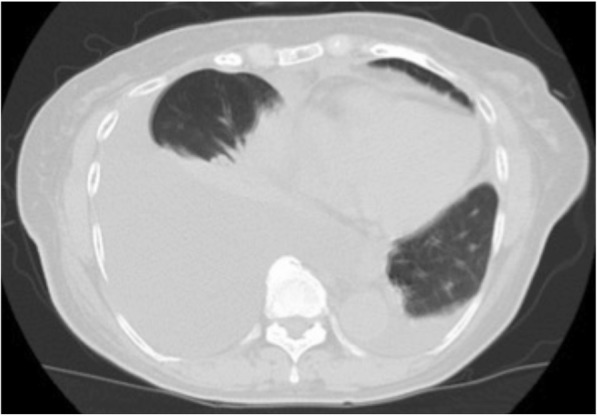
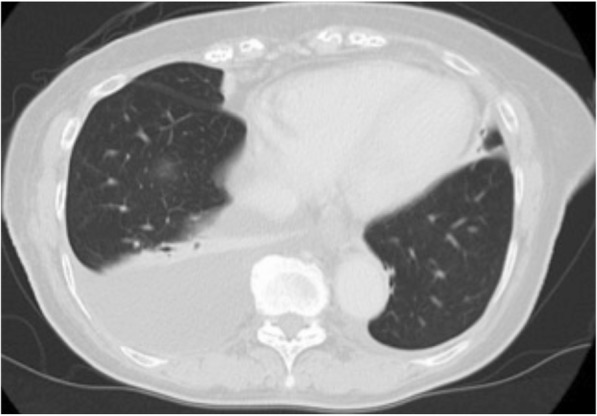
Case presentation: A 74-year-old Japanese woman presented with jaundice. She was diagnosed as having hilar cholangiocarcinoma and underwent right hepatectomy, caudate lobectomy, extrahepatic bile duct resection, and lymph node dissection after preoperative percutaneous transhepatic portal vein embolization. Postoperative liver function was normal. She developed chylous ascites on postoperative day 5, for which conservative treatment was initially effective. Dyspnea developed suddenly on postoperative day 42, and she had a massive right pleural effusion and a small amount of ascites. Management with pleural drainage, total parenteral nutrition, and octreotide injections decreased the chylothorax. However, the chylous effusion reaccumulated on postoperative day 57. As conservative treatments ultimately failed, lymphangiography was performed on postoperative day 62. Lymphangiography with Lipiodol (ethiodized oil) revealed extravasation into the pleural space, but the location of the leak was not identified. There was neither obstruction nor dilation of the thoracic duct. A lymphatic leak in her abdominal cavity was not demonstrated. A chest tube was placed after lymphangiography, and the chylothorax was diminished by postoperative day 71. She was discharged on postoperative day 72. Two and a half years after surgery, she is doing well with no evidence of recurrence of either chylothorax or cancer.
Conclusions: Chylothorax can occur after hepatectomy and pleural effusion should raise suspicion for chylothorax. Lymphangiography may be effective for both diagnosis and treatment in the case of chylothorax after hepatectomy.
Keywords: Abdominal surgery; Cholangiocarcinoma; Chylothorax; Hepatectomy; Lymphangiography.
Conflict of interest statement
Ethics approval and consent to participate
Our institutional ethics committee approved the publication of this case report.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
