

Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies
- PMID: 30475962
- PMCID: PMC6250988
- DOI: 10.1093/ajcn/nqy097
Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies
Abstract
Background: High dietary intake or blood concentrations (as biomarkers of dietary intake) of vitamin C, carotenoids, and vitamin E have been associated with reduced risk of cardiovascular disease, cancer, and mortality, but these associations have not been systematically assessed.
Objective: We conducted a systematic review and meta-analysis of prospective studies of dietary intake and blood concentrations of vitamin C, carotenoids, and vitamin E in relation to these outcomes.
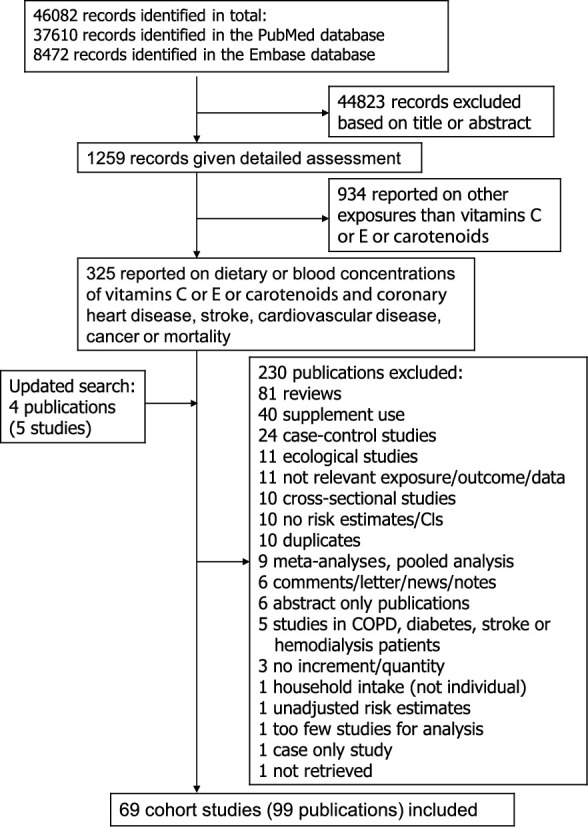
Design: We searched PubMed and Embase up to 14 February 2018. Summary RRs and 95% CIs were calculated with the use of random-effects models.
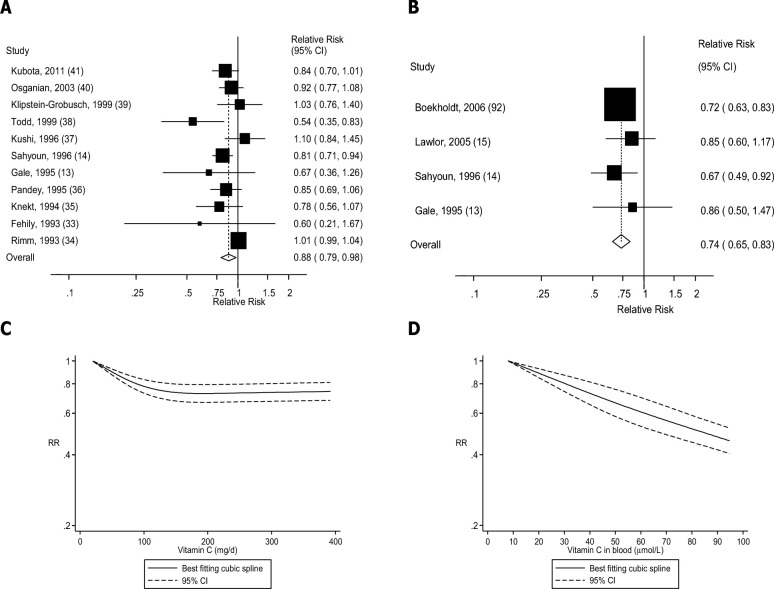
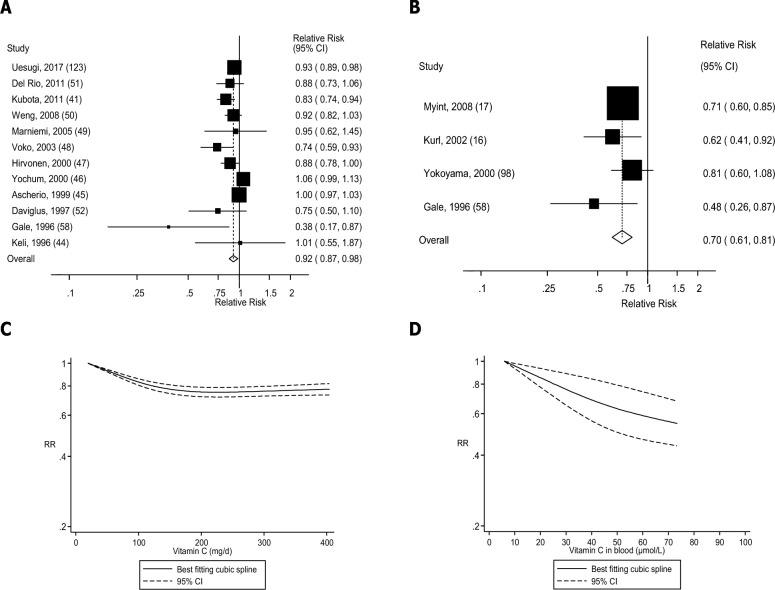
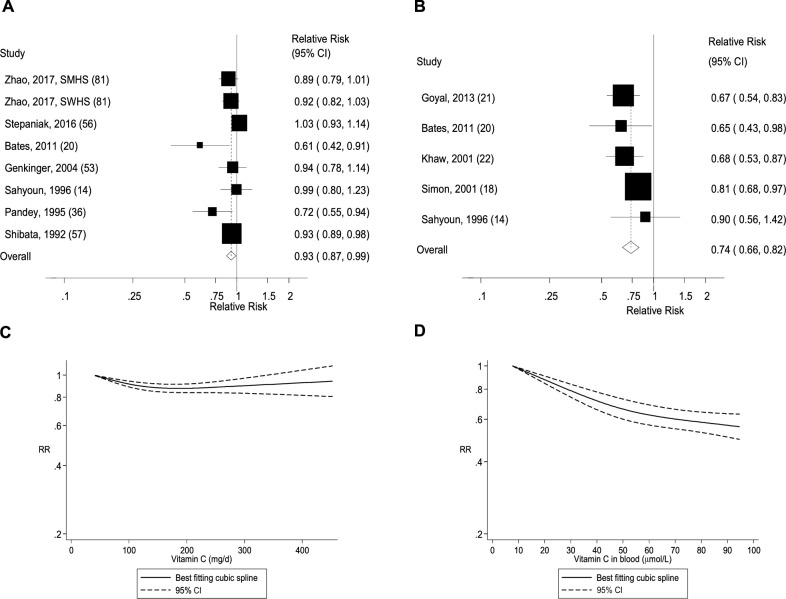
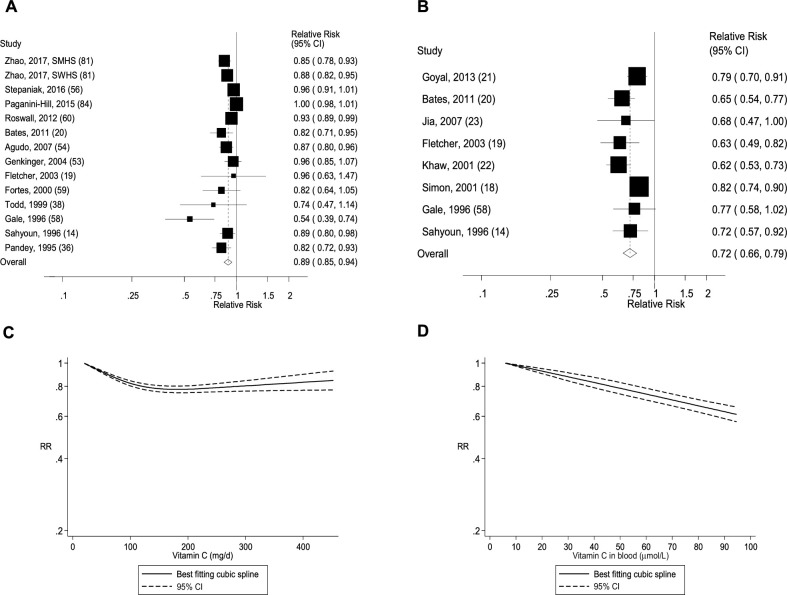
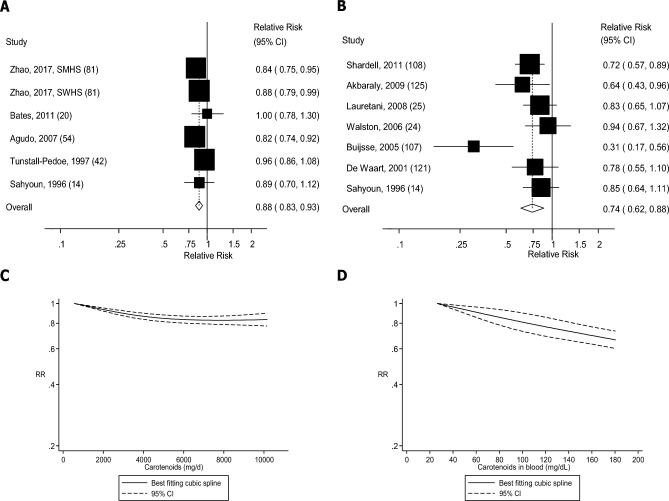
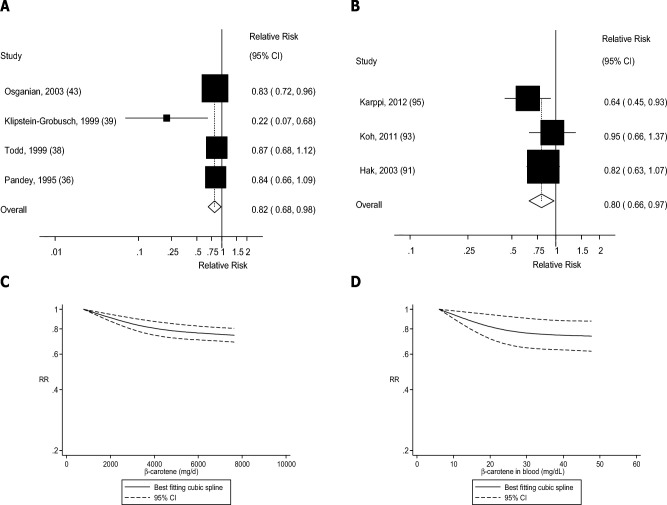
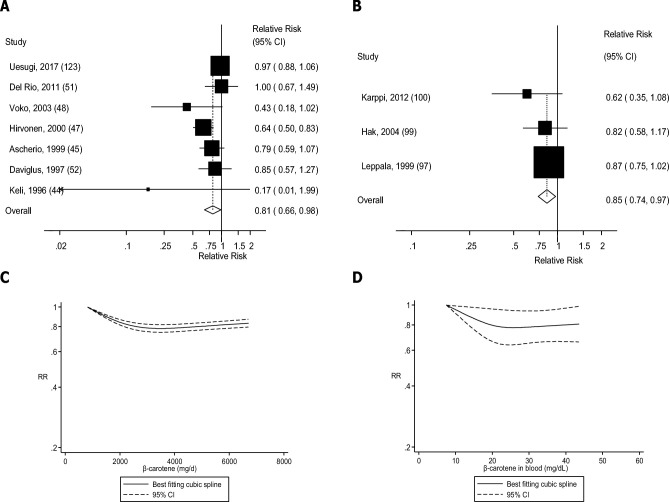
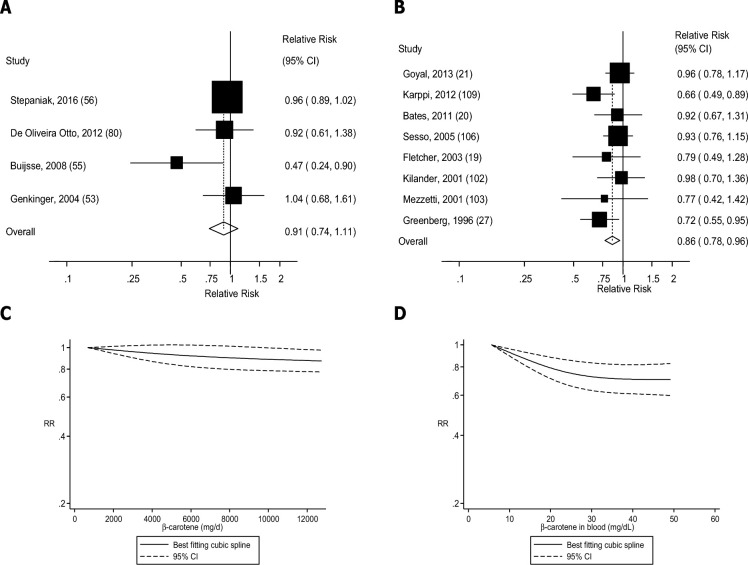
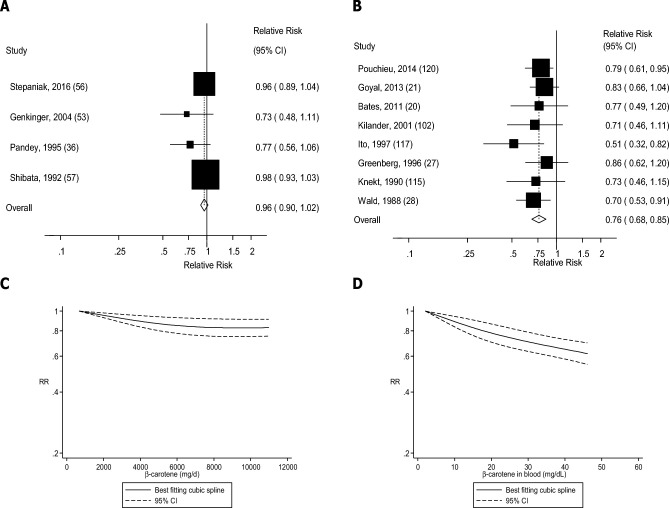
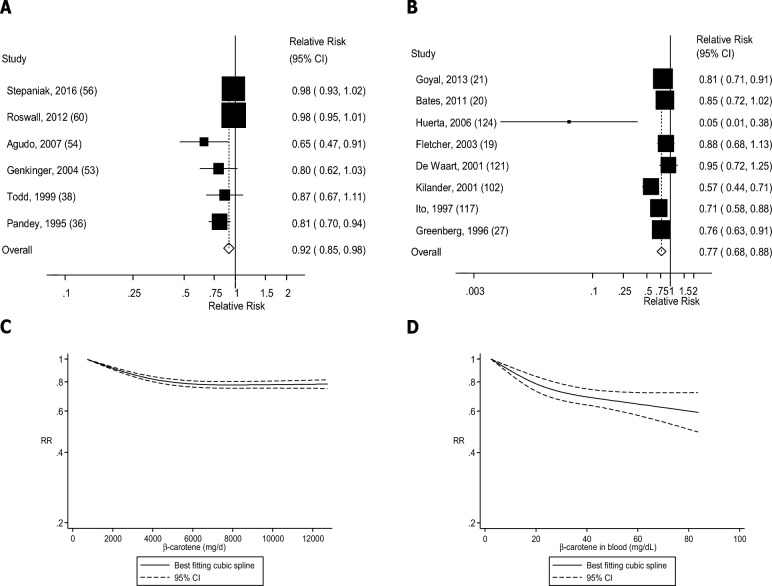
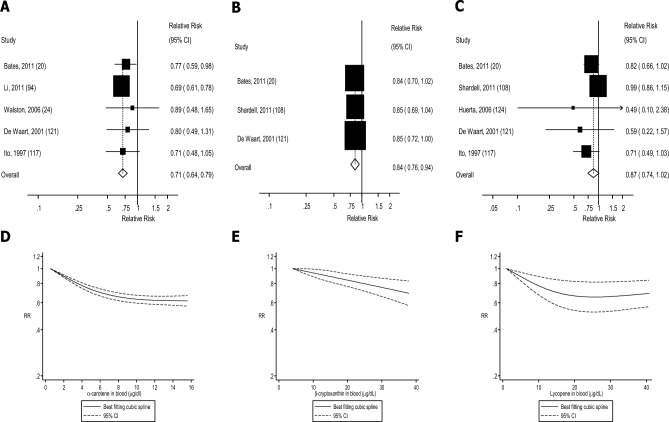
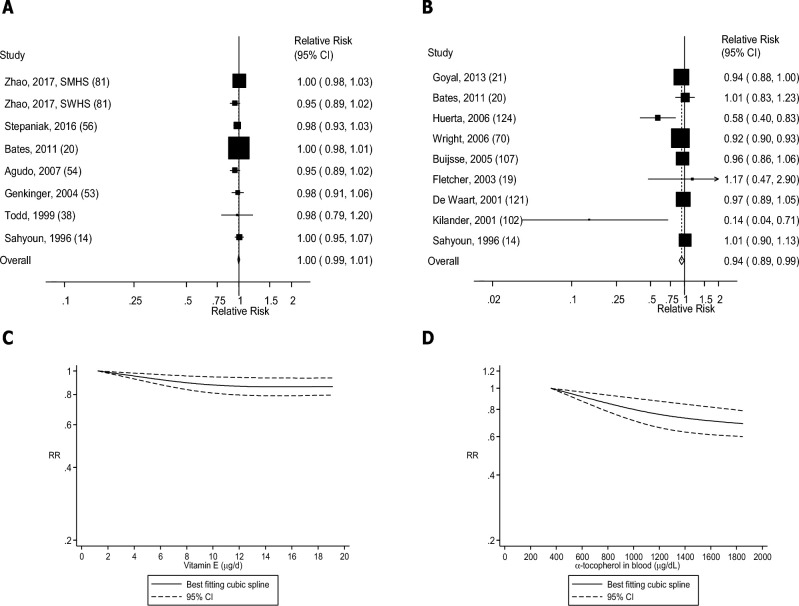
Results: Sixty-nine prospective studies (99 publications) were included. The summary RR per 100-mg/d increment of dietary vitamin C intake was 0.88 (95% CI: 0.79, 0.98, I2 = 65%, n = 11) for coronary heart disease, 0.92 (95% CI: 0.87, 0.98, I2 = 68%, n = 12) for stroke, 0.89 (95% CI: 0.85, 0.94, I2 = 27%, n = 10) for cardiovascular disease, 0.93 (95% CI: 0.87, 0.99, I2 = 46%, n = 8) for total cancer, and 0.89 (95% CI: 0.85, 0.94, I2 = 80%, n = 14) for all-cause mortality. Corresponding RRs per 50-μmol/L increase in blood concentrations of vitamin C were 0.74 (95% CI: 0.65, 0.83, I2 = 0%, n = 4), 0.70 (95% CI: 0.61, 0.81, I2 = 0%, n = 4), 0.76 (95% CI: 0.65, 0.87, I2 = 56%, n = 6), 0.74 (95% CI: 0.66, 0.82, I2 = 0%, n = 5), and 0.72 (95% CI: 0.66, 0.79, I2 = 0%, n = 8). Dietary intake and/or blood concentrations of carotenoids (total, β-carotene, α-carotene, β-cryptoxanthin, lycopene) and α-tocopherol, but not dietary vitamin E, were similarly inversely associated with coronary heart disease, stroke, cardiovascular disease, cancer, and/or all-cause mortality.
Conclusions: Higher dietary intake and/or blood concentrations of vitamin C, carotenoids, and α-tocopherol (as markers of fruit and vegetable intake) were associated with reduced risk of cardiovascular disease, total cancer, and all-cause mortality. These results support recommendations to increase fruit and vegetable intake, but not antioxidant supplement use, for chronic disease prevention.
Figures

References
-
- Leenders M, Sluijs I, Ros MM, Boshuizen HC, Siersema PD, Ferrari P, Weikert C, Tjonneland A, Olsen A, Boutron-Ruault MC et al.. Fruit and vegetable consumption and mortality: European Prospective Investigation into Cancer and Nutrition. Am J Epidemiol 2013;178:590–602. - PubMed
-
- Boffetta P, Couto E, Wichmann J, Ferrari P, Trichopoulos D, Bueno-de-Mesquita HB, van Duijnhoven FJ, Buchner FL, Key T, Boeing H et al.. Fruit and vegetable intake and overall cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). J Natl Cancer Inst 2010;102:529–37. - PubMed
-
- Aune D, Lau R, Chan DS, Vieira R, Greenwood DC, Kampman E, Norat T. Nonlinear reduction in risk for colorectal cancer by fruit and vegetable intake based on meta-analysis of prospective studies. Gastroenterology 2011;141:106–18. - PubMed
-
- Aune D, Chan DS, Vieira AR, Rosenblatt DA, Vieira R, Greenwood DC, Norat T. Fruits, vegetables and breast cancer risk: a systematic review and meta-analysis of prospective studies. Breast Cancer Res Treat 2012;134:479–93. - PubMed
