

Equalization of four cardiovascular risk algorithms after systematic recalibration: individual-participant meta-analysis of 86 prospective studies
- PMID: 30476079
- PMCID: PMC6374687
- DOI: 10.1093/eurheartj/ehy653
Equalization of four cardiovascular risk algorithms after systematic recalibration: individual-participant meta-analysis of 86 prospective studies
Abstract
Aims: There is debate about the optimum algorithm for cardiovascular disease (CVD) risk estimation. We conducted head-to-head comparisons of four algorithms recommended by primary prevention guidelines, before and after 'recalibration', a method that adapts risk algorithms to take account of differences in the risk characteristics of the populations being studied.
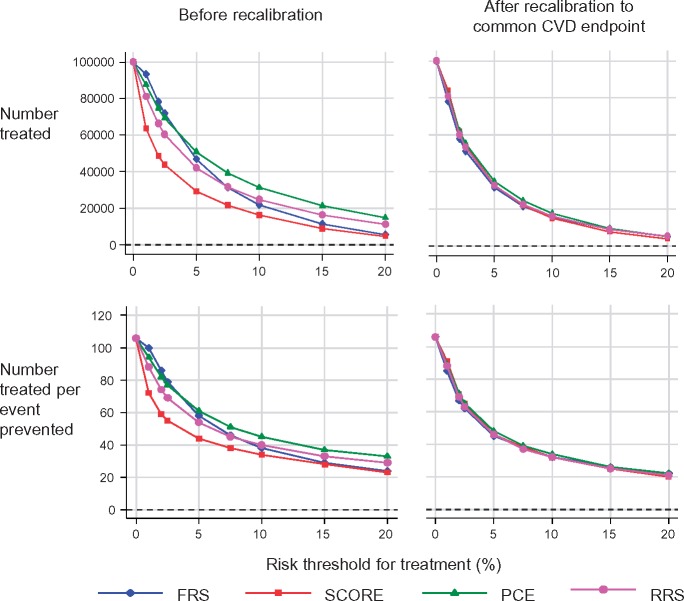
Methods and results: Using individual-participant data on 360 737 participants without CVD at baseline in 86 prospective studies from 22 countries, we compared the Framingham risk score (FRS), Systematic COronary Risk Evaluation (SCORE), pooled cohort equations (PCE), and Reynolds risk score (RRS). We calculated measures of risk discrimination and calibration, and modelled clinical implications of initiating statin therapy in people judged to be at 'high' 10 year CVD risk. Original risk algorithms were recalibrated using the risk factor profile and CVD incidence of target populations. The four algorithms had similar risk discrimination. Before recalibration, FRS, SCORE, and PCE over-predicted CVD risk on average by 10%, 52%, and 41%, respectively, whereas RRS under-predicted by 10%. Original versions of algorithms classified 29-39% of individuals aged ≥40 years as high risk. By contrast, recalibration reduced this proportion to 22-24% for every algorithm. We estimated that to prevent one CVD event, it would be necessary to initiate statin therapy in 44-51 such individuals using original algorithms, in contrast to 37-39 individuals with recalibrated algorithms.
Conclusion: Before recalibration, the clinical performance of four widely used CVD risk algorithms varied substantially. By contrast, simple recalibration nearly equalized their performance and improved modelled targeting of preventive action to clinical need.
Keywords: Calibration; Cardiovascular disease; Discrimination; Risk algorithms; Risk prediction.
© The Author(s) 2018. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures




Comment in
-
Is 're-calibration' of standard cardiovascular disease (CVD) risk algorithms the panacea to improved CVD risk prediction and prevention?Eur Heart J. 2019 Feb 14;40(7):632-634. doi: 10.1093/eurheartj/ehy726. Eur Heart J. 2019. PMID: 30476017 No abstract available.
References
-
- US Preventive Services Task Force. Statin use for the primary prevention of cardiovascular disease in adults: US preventive services task force recommendation statement. JAMA 2016;316:1997–2007. - PubMed
-
- Cooney MT, Dudina A, D’Agostino R, Graham IM.. Cardiovascular risk-estimation systems in primary prevention: do they differ? Do they make a difference? Can we see the future? Circulation 2010;122:300–310. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC, Watson K, Wilson PWF.. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;129:S1–S45. - PubMed
-
- Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O’Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC, Sorlie P, Stone NJ, Wilson PWF.. 2013 ACC/AHA guideline on the assessment of cardiovascular risk. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;129:S49–S73. - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney M-T, Corrà U, Cosyns B, Deaton C, Graham I, Hall MS, Hobbs FDR, Løchen M-L, Löllgen H, Marques-Vidal P, Perk J, Prescott E, Redon J, Richter DJ, Sattar N, Smulders Y, Tiberi M, van der Worp HB, van Dis I, Verschuren WMM, Binno S, De BG, Roffi M, Aboyans V, Bachl N, Bueno H, Carerj S, Cho L, Cox J, De SJ, Egidi G, Fisher M, Fitzsimons D, Franco OH, Guenoun M, Jennings C, Jug B, Kirchhof P, Kotseva K, Lip GYH, Mach F, Mancia G, Bermudo FM, Mezzani A, Niessner A, Ponikowski P, Rauch B, Rydén L, Stauder A, Turc G, Wiklund O, Windecker S, Zamorano JL, Zamorano JL, Aboyans V, Achenbach S, Agewall S, Badimon L, Barón EG, Baumgartner H, Bax JJ, Bueno H, Carerj S, Dean V, Erol Ç FD, Gaemperli O, Kirchhof P, Kolh P, Lancellotti P, Lip GYH, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Roffi M, Torbicki A, Carneiro AV, Windecker S, Metzler B, Najafov R, Stelmashok V, De MC, Dilić M, Gruev I, Miličić D, Vaverkova H, Gustafsson I, Attia I, Duishvili D, Ferrières J, Kostova N, Klimiashvili Z, Hambrecht R, Tsioufis K, Szabados E, Andersen K, Vaughan C, Zafrir B, Novo S, Davletov K, Jashari F, Kerimkulova A, Mintale I, Saade G, Petrulioniene Z, Delagardelle C, Magri CJ, Rudi V, Oukerraj L, Çölkesen BE, Schirmer H, dos RRP, Gherasim D, Nedogoda S, Zavatta M, Giga V, Filipova S, Padial LR, Kiessling A, Mach F, Mahdhaoui A, Ural D, Nesukay E, Gale C.. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016;37:2315–2381. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- SP/09/002/BHF_/British Heart Foundation/United Kingdom
- G0800270/MRC_/Medical Research Council/United Kingdom
- RG/13/13/30194/BHF_/British Heart Foundation/United Kingdom
- MC_UU_12011/2/MRC_/Medical Research Council/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- 14136/CRUK_/Cancer Research UK/United Kingdom
- G0401527/MRC_/Medical Research Council/United Kingdom
- CH/12/2/29428/BHF_/British Heart Foundation/United Kingdom
- G0701619/MRC_/Medical Research Council/United Kingdom
- R01 HL109284/HL/NHLBI NIH HHS/United States
- G0400491/MRC_/Medical Research Council/United Kingdom
- RG/13/2/30098/BHF_/British Heart Foundation/United Kingdom
- MR/R024227/1/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1015/MRC_/Medical Research Council/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- MC_UU_12023/21/MRC_/Medical Research Council/United Kingdom
- MR/N003284/1/MRC_/Medical Research Council/United Kingdom
- P30 ES005605/ES/NIEHS NIH HHS/United States
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MC_UU_00002/7/MRC_/Medical Research Council/United Kingdom
- RG/16/11/32334/BHF_/British Heart Foundation/United Kingdom
- 19583/VAC_/Versus Arthritis/United Kingdom
- 268834/ERC_/European Research Council/International
- 10/33/04/DH_/Department of Health/United Kingdom
- MR/K013351/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- 204623/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- RG/13/16/30528/BHF_/British Heart Foundation/United Kingdom
- G0601019/MRC_/Medical Research Council/United Kingdom
- MC_UU_12013/5/MRC_/Medical Research Council/United Kingdom
- 001/WHO_/World Health Organization/International
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- MR/K014811/1/MRC_/Medical Research Council/United Kingdom
