

Upfront Magnetic Resonance Imaging-Guided Stereotactic Laser-Ablation in Newly Diagnosed Glioblastoma: A Multicenter Review of Survival Outcomes Compared to a Matched Cohort of Biopsy-Only Patients
- PMID: 30476325
- PMCID: PMC7054708
- DOI: 10.1093/neuros/nyy449
Upfront Magnetic Resonance Imaging-Guided Stereotactic Laser-Ablation in Newly Diagnosed Glioblastoma: A Multicenter Review of Survival Outcomes Compared to a Matched Cohort of Biopsy-Only Patients
Abstract
Background: Laser ablation (LA) is used as an upfront treatment in patients with deep seated newly diagnosed Glioblastoma (nGBM).
Objective: To evaluate the outcomes of LA in patients with nGBM and compare them with a matched biopsy-only cohort.
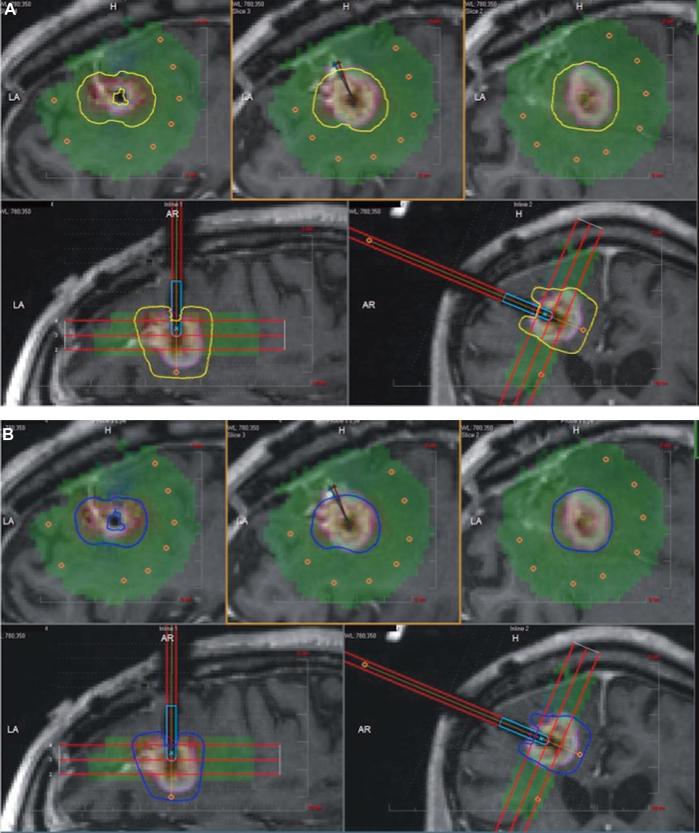
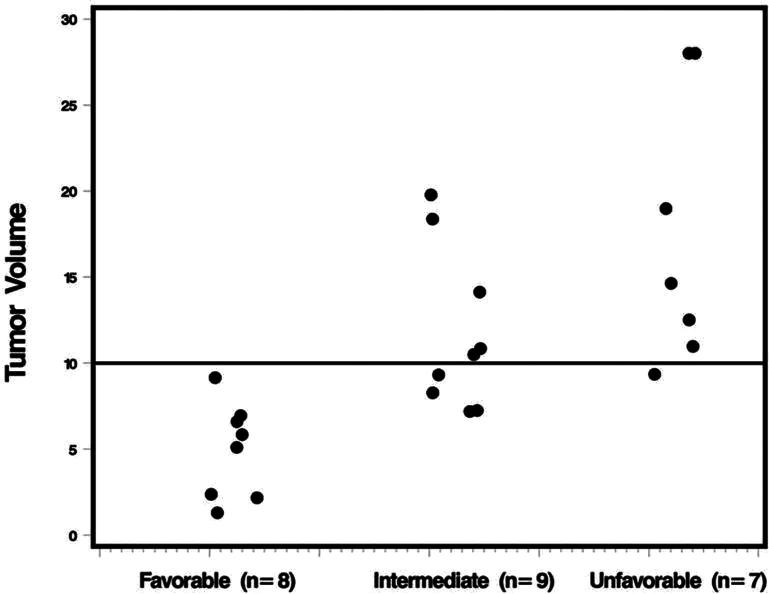
Methods: Twenty-four nGBM patients underwent upfront LA at Cleveland clinic, Washington University in St. Louis, and Yale University (6/2011-12/2014) followed by chemo/radiotherapy. Also, 24 out of 171 nGBM patients with biopsy followed by chemo/radiotherapy were matched based on age (< 70 vs ≥ 70), gender, tumor location (deep vs lobar), and volume (<11 cc vs ≥11 cc). Progression-free survival (PFS), overall survival (OS), and disease-specific PFS and OS were outcome measures. Three prognostic groups were identified based on extent of tumor ablation by thermal-damage-threshold (TDT)-lines.
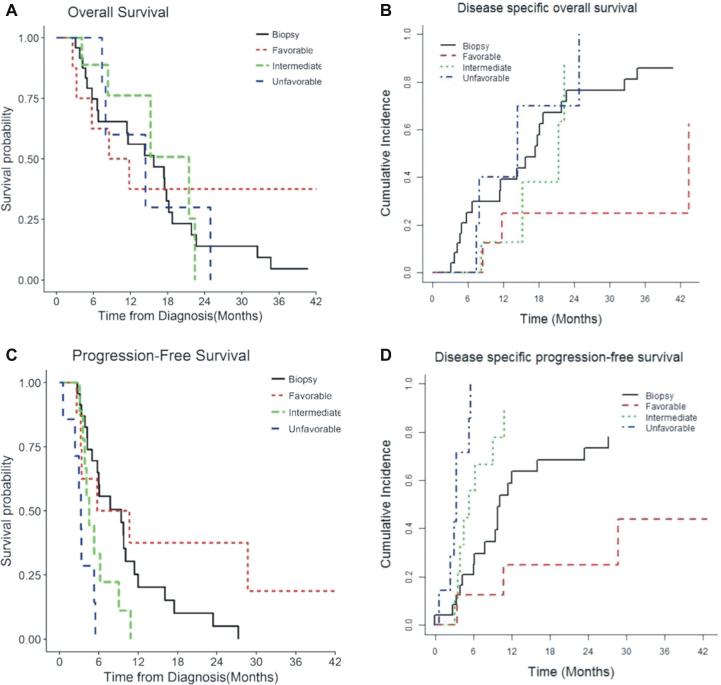
Results: The median tumor volume in LA (n = 24) and biopsy only (n = 24) groups was 9.3 cm3 and 8.2 cm3 respectively. Overall, median estimate of OS and PFS in LA cohort was 14.4 and 4.3 mo compared to 15.8 mo and 5.9 mo for biopsy only cohort. On multivariate analysis, favorable TDT-line prognostic groups were associated with lower incidence of disease specific death (P = .03) and progression (P = .05) compared to other groups including biopsy only cohort. Only age (<70 yr, P = .02) and tumor volume (<11 cc, P = .03) were favorable prognostic factors for OS.
Conclusion: The maximum tumor coverage by LA followed by radiation/chemotherapy is an effective treatment modality in patients with nGBM, compared to biopsy only cohort. The TDT-line prognostic groups were independent predictor of disease specific death and progression after LA.
Keywords: Brain tumor; GBM; LITT; Minimally invasive; NeuroBlate; Novel treatment.
Copyright © 2018 by the Congress of Neurological Surgeons.
Figures
References
-
- Omuro A, DeAngelis LM. Glioblastoma and other malignant gliomas: a clinical review. JAMA. 2013;310(17):1842–1850. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ et al.. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Andersen AP. Postoperative irradiation of glioblastomas: Results in a randomized series. Acta Radiol Oncol Radiat Phys Biol. 1978;17(6):475–484. - PubMed
-
- Walker MD, Alexander E Jr., Hunt WE et al.. Evaluation of BCNU and/or radiotherapy in the treatment of anaplastic gliomas. A cooperative clinical trial. J Neurosurg. 1978;49(3):333–343. - PubMed
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359(5):492–507. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
