

Interventions to reduce readmissions: can complex adaptive system theory explain the heterogeneity in effectiveness? A systematic review
- PMID: 30477576
- PMCID: PMC6260570
- DOI: 10.1186/s12913-018-3712-7
Interventions to reduce readmissions: can complex adaptive system theory explain the heterogeneity in effectiveness? A systematic review
Abstract
Background: Successfully transitioning patients from hospital to home is a complex, often uncertain task. Despite significant efforts to improve the effectiveness of care transitions, they remain a challenge across health care systems. The lens of complex adaptive systems (CAS) provides a theoretical approach for studying care transition interventions, with potential implications for intervention effectiveness. The aim of this study is to examine whether care transition interventions that are congruent with the complexity of the processes and conditions they are trying to improve will have better outcomes.
Methods: We identified a convenience sample of high-quality care transition intervention studies included in a care transition synthesis report by Kansagara and colleagues. After excluding studies that did not meet our criteria, we scored each study based on (1) the presence or absence of 5 CAS characteristics (learning, interconnections, self-organization, co-evolution, and emergence), as well as system-level interdependencies (resources and processes) in the intervention design, and (2) scored study readmission-related outcomes for effectiveness.
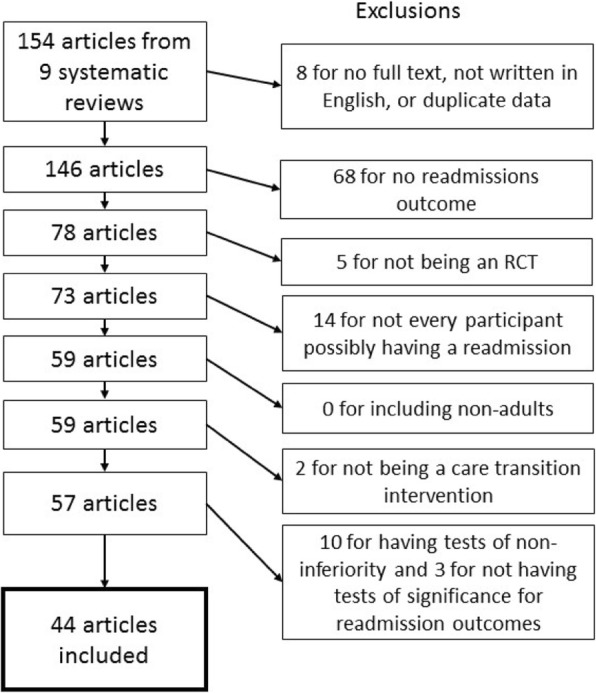
Results: Forty-four of the 154 reviewed articles met our inclusion criteria; these studies reported on 46 interventions. Nearly all the interventions involved a change in interconnections between people compared with care as usual (96% of interventions), and added resources (98%) and processes (98%). Most contained elements impacting learning (67%) and self-organization (69%). No intervention reflected either co-evolution or emergence. Almost 40% of interventions were rated as effective in terms of impact on hospital readmissions. Chi square testing for an association between outcomes and CAS characteristics was not significant for learning or self-organization, however interventions rated as effective were significantly more likely to have both of these characteristics (78%) than interventions rated as having no effect (32%, p = 0.005).
Conclusions: Interventions with components that influenced learning and self-organization were associated with a significant improvement in hospital readmissions-related outcomes. Learning alone might be necessary but not be sufficient for improving transitions. However, building self-organization into the intervention might help people effectively respond to problems and adapt in uncertain situations to reduce the likelihood of readmission.
Keywords: Care transitions; Complex adaptive systems; Health care interventions; Hospital readmissions; Patient education; Self-organization.
Conflict of interest statement
Authors’ information
Not applicable
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors have no competing interests to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Kansagara D, Chiovaro JC, Kagen D, Jencks S, Rhyne K, O’Neil M, et al. Transitions of care from hospital to home: a summary of systematic evidence reviews and recommendations for transitional care in the veterans health administration: Department of Veterans Affairs; 2015. https://www.ncbi.nlm.nih.gov/books/NBK311349/. - PubMed
-
- Naylor Mary D., Shaid Elizabeth C., Carpenter Deborah, Gass Brianna, Levine Carol, Li Jing, Malley Ann, McCauley Kathleen, Nguyen Huong Q., Watson Heather, Brock Jane, Mittman Brian, Jack Brian, Mitchell Suzanne, Callicoatte Becky, Schall John, Williams Mark V. Components of Comprehensive and Effective Transitional Care. Journal of the American Geriatrics Society. 2017;65(6):1119–1125. doi: 10.1111/jgs.14782. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
