

Epidemiology of status epilepticus in adults: A population-based study on incidence, causes, and outcomes
- PMID: 30478910
- PMCID: PMC7380005
- DOI: 10.1111/epi.14607
Epidemiology of status epilepticus in adults: A population-based study on incidence, causes, and outcomes
Abstract
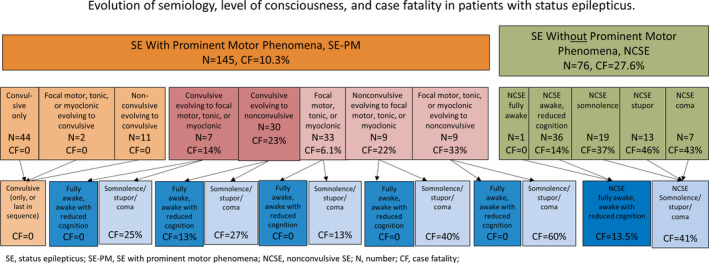
Objective: In 2015, the International League Against Epilepsy (ILAE) proposed a new definition of status epilepticus (SE): 5 minutes of ongoing seizure activity to diagnose convulsive SE (CSE, ie, bilateral tonic-clonic SE) and 10 minutes for focal SE and absence SE, rather than the earlier criterion of 30 minutes. Based on semiology, several types of SE with prominent motor phenomena at any time (including CSE) were distinguished from those without (ie, nonconvulsive SE, NCSE). We present the first population-based incidence study applying the new 2015 ILAE definition and classification of SE and report the impact of the evolution of semiology and level of consciousness (LOC) on outcome.
Methods: We conducted a retrospective population-based incidence study of all adult patients with SE residing in the city of Salzburg between January 2011 and December 2015. Patients with hypoxic encephalopathy were excluded. SE was defined and classified according to the ILAE 2015.
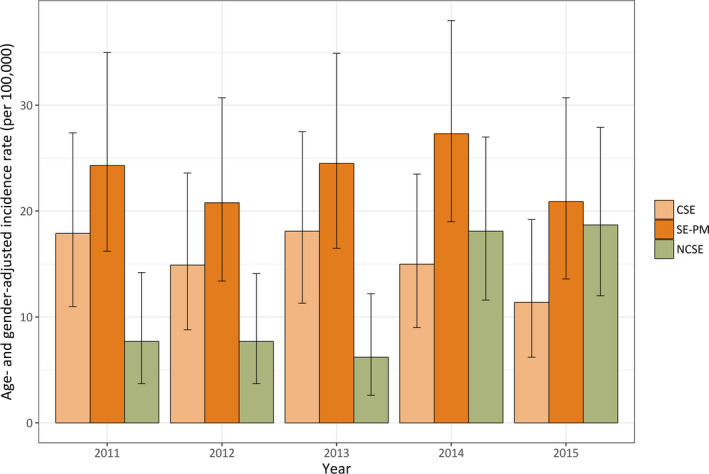
Results: We identified 221 patients with a median age of 69 years (range 20-99 years). The age- and sex-adjusted incidence of a first episode of SE, NCSE, and SE with prominent motor phenomena (including CSE) was 36.1 (95% confidence interval [CI] 26.2-48.5), 12.1 (95% CI 6.8-20.0), and 24.0 (95% CI 16.0-34.5; including CSE 15.8 [95% CI 9.4-24.8]) per 100 000 adults per year, respectively. None of the patients whose SE ended with or consisted of only bilateral tonic-clonic activity died. In all other clinical presentations, case fatality was lower in awake patients (8.2%) compared with patients with impaired consciousness (33%).
Significance: This first population-based study using the ILAE 2015 definition and classification of SE found an increase of incidence of 10% compared to previous definitions. We also provide epidemiologic evidence that different patterns of status evolution and LOCs have strong prognostic implications.
Keywords: classification; epidemiology; evolution; incidence; semiology; status epilepticus.
© 2018 The Authors. Epilepsia published by Wiley Periodicals, Inc. on behalf of International League Against Epilepsy.
Conflict of interest statement
Markus Leitinger reports grants from Medtronic and UCB Pharma and personal fees from Everpharma and Eisai. Eugen Trinka reports personal fees from Eisai, personal fees from Everpharma, grants and personal fees from Biogen Idec, personal fees from Medtronics, personal fees from Bial, personal fees from Newbridge, grants and personal fees from UCB Pharma and Eisai, personal fees from GL Pharma, personal fees from GlaxoSmithKline, personal fees from Boehringer, personal fees from Viropharma and Actavis, grants from Red Bull, grants from Merck, grants from European Union, grants from FWF Österreichischer Fond zur Wissenschaftsförderung, grants from Bundesministerium für Wissenschaft und Forschung, and grants from the Jubiläumsfond der Österreichischen Nationalbank, outside the submitted work. Georg Zimmermann reports financial support from an Investigator‐Initiated Study grant from Eisai Ltd. (FYC‐IIS‐0M044‐1023) to Paracelsus Medical University, not related to the present work. Alexandra Rohracher reports travel support and speaker’s honoraria from Eisai. Gudrun Kalss reports travel support by UCB, Eisai, OEGN (Austrian Society of Neurology), Cyberonics, the Asian Oceanian Association of Neurology, CEA, and ILAE. Caroline Neuray reports speaker′s honoraria and travel expenses from Eisai. Julia Höfler reports speaker’s honoraria from UCB and travel grants from UCB, Eisai, and Gerot‐Lannach. Giorgi Kuchukhidze has received travel support from Eisai and UCB Pharma. Judith Dobesberger has received honoraria and travel support from UCB Pharma, Gerot‐Lannach, Eisai, GlaxoSmithKline, and Neurodata GmbH/Micromed Austria. Helmut F. Novak has received speaker’s honoraria from Baxter Austria, Astellas Pharma, SCS‐Angelini Pharmaceuticals, Fresenius Medical Care Austria and Orion Pharma, from UCB Pharma for clinical medication monitoring, travel grants from Fresenius Kabi Austria and as consultant to Hayward Medical Communications. Stefano Meletti reports personal fees as a scientific advisory board member for UCB and EISAI. Giada Giovannini, Christina Florea, Rudolf Kreidenhuber, Claudia Granbichler, Georg Pilz and Uwe Siebert report no disclosure. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures
References
-
- Neligan A, Shorvon SD. Frequency and prognosis of convulsive status epilepticus of different causes: a systematic review. Arch Neurol. 2010;67:931–40. - PubMed
-
- Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus—Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia. 2015;56:1515–23. - PubMed
-
- DeLorenzo RJ, Hauser WA, Towne AR, et al. A prospective, population‐based epidemiologic study of status epilepticus in Richmond, Virginia. Neurology. 1996;46:1029–35. - PubMed
-
- Hesdorffer DC, Logroscino G, Cascino G, Annegers JF, Hauser WA. Incidence of status epilepticus in Rochester, Minnesota, 1965‐1984. Neurology. 1998;50:735–41. - PubMed
-
- Logroscino G, Hesdorffer DC, Cascino G, Annegers JF, Hauser WA. Time trends in incidence, mortality, and case‐fatality after first episode of status epilepticus. Epilepsia. 2001;42:1031–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
