

The prognostic significance of estrogen and progesterone receptors in grade I and II endometrioid endometrial adenocarcinoma: hormone receptors in risk stratification
- PMID: 30479097
- PMCID: PMC6304404
- DOI: 10.3802/jgo.2019.30.e13
The prognostic significance of estrogen and progesterone receptors in grade I and II endometrioid endometrial adenocarcinoma: hormone receptors in risk stratification
Abstract
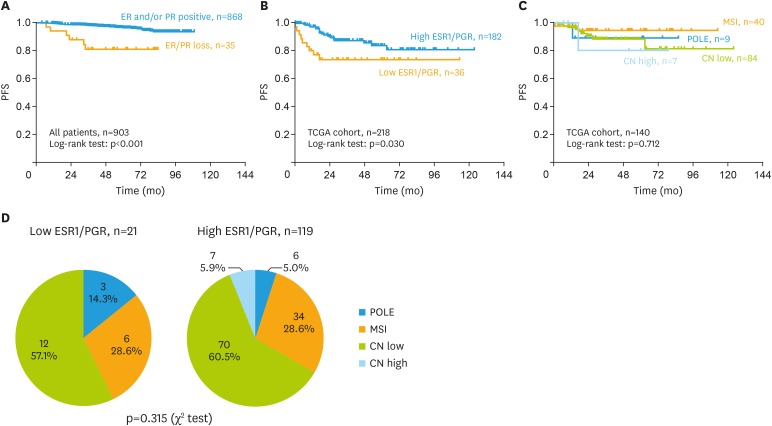
Objectives: Although patients with grade I and II endometrioid endometrial adenocarcinoma (EEA) are considered with good prognosis, among them 15%-25% died in 5 years. It is still unknown whether integrating estrogen receptor (ER) and progesterone receptor (PR) into clinical risk stratification can help select high-risk patients with grade I-II EEA. This study was to investigate the prognostic value of ER and PR double negativity (ER/PR loss) in grade I-II EEA, and the association between ER/PR loss and The Cancer Genome Atlas (TCGA) classification.
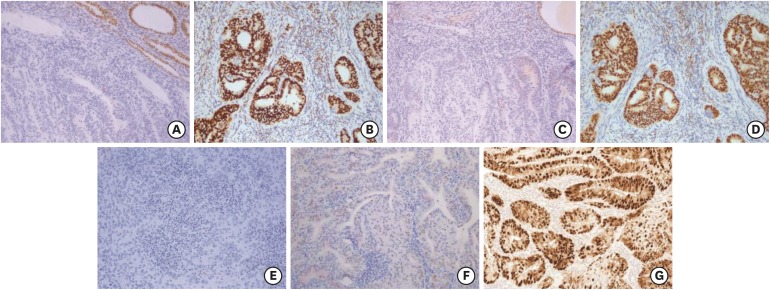
Methods: ER and PR were assessed by immunohistochemistry on hysterectomy specimens of 903 patients with grade I-II EEA. ER and PR negativity were determined when <1% tumor nuclei were stained. Gene expression data were obtained from the TCGA research network.
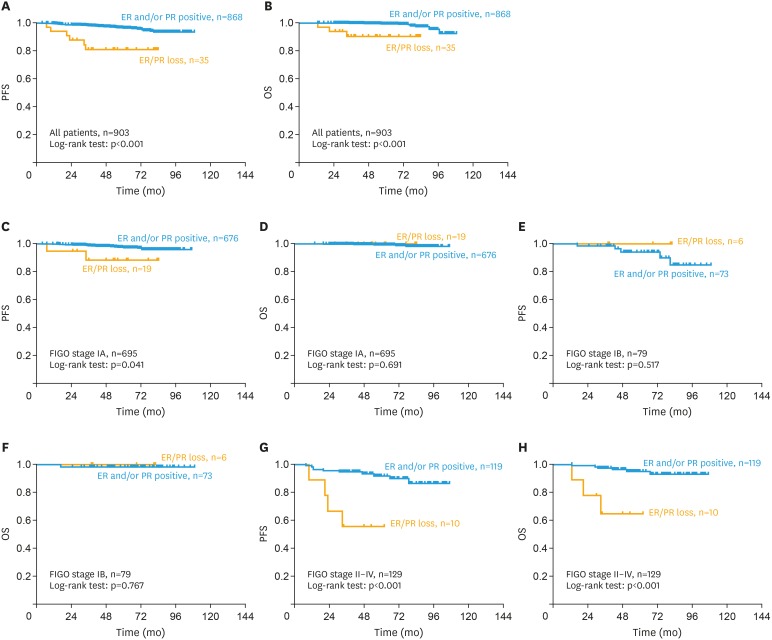
Results: Compared with ER or PR positive patients (n=868), patients with ER/PR loss (n=35) had deeper myometrial infiltration (p=0.012), severer FIGO stage (p=0.004), and higher rate of pelvic lymph node metastasis (p=0.020). In univariate analysis, ER/PR loss correlated with a shorter progression-free survival (PFS; hazard ratio [HR]=5.25; 95% confidence interval [CI]=2.21-12.52) and overall survival (OS; HR=7.59; 95% CI=2.55-22.60). In multivariate analysis, ER/PR loss independently predicted poor PFS (HR=3.77; 95% CI=1.60-10.14) and OS (HR=5.56; 95% CI=1.37-22.55) for all patients, and poor PFS for patients in stage IA (n=695; HR=5.54; 95% CI=1.28-23.89) and stage II-IV (n=129; HR=5.77; 95% CI=1.57-21.27). No association was found between ER/PR loss and TCGA classification.
Conclusion: Integrating ER/PR evaluation into clinical risk stratification may improve prognosis for grade I-II EEA patients.
Keywords: Biomarker; Endometrial Cancer; Endometrioid Carcinoma; Estrogen Receptor; Low-Grade; Progesterone Receptor.
Copyright © 2019. Asian Society of Gynecologic Oncology, Korean Society of Gynecologic Oncology.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Progesterone receptor negativity is an independent risk factor for relapse in patients with early stage endometrioid endometrial adenocarcinoma.Gynecol Oncol. 2013 Sep;130(3):463-9. doi: 10.1016/j.ygyno.2013.06.015. Epub 2013 Jun 15. Gynecol Oncol. 2013. PMID: 23777659
-
[The value of progesterone and estrogen receptors expression in tissue microarray method in prognosis of patients with endometrioid endometrial cancer].Ginekol Pol. 2013 Feb;84(2):95-101. doi: 10.17772/gp/1547. Ginekol Pol. 2013. PMID: 23668054 Polish.
-
Hormone receptor loss in endometrial carcinoma curettage predicts lymph node metastasis and poor outcome in prospective multicentre trial.Eur J Cancer. 2013 Nov;49(16):3431-41. doi: 10.1016/j.ejca.2013.06.016. Epub 2013 Aug 8. Eur J Cancer. 2013. PMID: 23932335 Clinical Trial.
-
Prognosis of polymerase epsilon (POLE) mutation in high-grade endometrioid endometrial cancer: Systematic review and meta-analysis.Gynecol Oncol. 2024 Mar;182:99-107. doi: 10.1016/j.ygyno.2024.01.018. Epub 2024 Jan 22. Gynecol Oncol. 2024. PMID: 38262245 Free PMC article.
-
TCGA molecular subgroups of endometrial carcinoma in ovarian endometrioid carcinoma: A quantitative systematic review.Gynecol Oncol. 2021 Nov;163(2):427-432. doi: 10.1016/j.ygyno.2021.08.011. Epub 2021 Aug 24. Gynecol Oncol. 2021. PMID: 34446267
Cited by
-
Mesonephric-Like Adenocarcinoma of the Endometrium: Diagnostic Advances to Spot This Wolf in Sheep's Clothing. A Review of the Literature.J Clin Med. 2021 Feb 11;10(4):698. doi: 10.3390/jcm10040698. J Clin Med. 2021. PMID: 33670088 Free PMC article. Review.
-
Endometrial carcinoma in a gravid uterus: a case report and literature review.BMC Pregnancy Childbirth. 2019 Nov 20;19(1):425. doi: 10.1186/s12884-019-2489-y. BMC Pregnancy Childbirth. 2019. PMID: 31747899 Free PMC article. Review.
-
Identification of key genes and pathways between type I and type II endometrial cancer using bioinformatics analysis.Oncol Lett. 2019 Sep;18(3):2464-2476. doi: 10.3892/ol.2019.10550. Epub 2019 Jun 28. Oncol Lett. 2019. PMID: 31452737 Free PMC article.
-
Expression of SUMO associated proteins in the mouse endometrium is regulated by ovarian hormones throughout the estrous cycle.Exp Ther Med. 2020 Mar;19(3):1855-1863. doi: 10.3892/etm.2020.8416. Epub 2020 Jan 3. Exp Ther Med. 2020. PMID: 32104241 Free PMC article.
-
Invasiveness of endometrial cancer cell lines is potentiated by estradiol and blocked by a traditional medicine Guizhi Fuling at clinically relevant doses.Front Oncol. 2023 Jan 16;12:1015708. doi: 10.3389/fonc.2022.1015708. eCollection 2022. Front Oncol. 2023. PMID: 36727068 Free PMC article.
References
-
- World Health Organization, International Agency for Research on Cancer. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012 [Internet] Lyon: International Agency for Re-search on Cancer; [cited 2018 Jun 1]. Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx.
-
- Kitchener HC, Trimble EL Endometrial Cancer Working Group of the Gynecologic Cancer Intergroup. Endometrial cancer state of the science meeting. Int J Gynecol Cancer. 2009;19:134–140. - PubMed
-
- Abeler VM, Kjørstad KE. Endometrial adenocarcinoma in Norway. A study of a total population. Cancer. 1991;67:3093–3103. - PubMed
-
- Dedes KJ, Wetterskog D, Ashworth A, Kaye SB, Reis-Filho JS. Emerging therapeutic targets in endometrial cancer. Nat Rev Clin Oncol. 2011;8:261–271. - PubMed
-
- Rose PG. Endometrial carcinoma. N Engl J Med. 1996;335:640–649. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
