

Validation and reproducibility of cardiovascular 4D-flow MRI from two vendors using 2 × 2 parallel imaging acceleration in pulsatile flow phantom and in vivo with and without respiratory gating
- PMID: 30479136
- PMCID: PMC6402051
- DOI: 10.1177/0284185118784981
Validation and reproducibility of cardiovascular 4D-flow MRI from two vendors using 2 × 2 parallel imaging acceleration in pulsatile flow phantom and in vivo with and without respiratory gating
Abstract
Background: 4D-flow magnetic resonance imaging (MRI) is increasingly used.
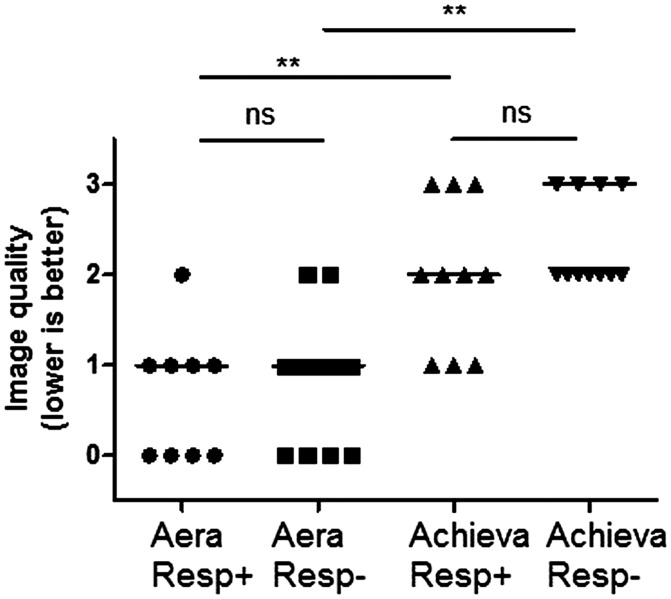
Purpose: To validate 4D-flow sequences in phantom and in vivo, comparing volume flow and kinetic energy (KE) head-to-head, with and without respiratory gating.
Material and methods: Achieva dStream (Philips Healthcare) and MAGNETOM Aera (Siemens Healthcare) 1.5-T scanners were used. Phantom validation measured pulsatile, three-dimensional flow with 4D-flow MRI and laser particle imaging velocimetry (PIV) as reference standard. Ten healthy participants underwent three cardiac MRI examinations each, consisting of cine-imaging, 2D-flow (aorta, pulmonary artery), and 2 × 2 accelerated 4D-flow with (Resp+) and without (Resp-) respiratory gating. Examinations were acquired consecutively on both scanners and one examination repeated within two weeks. Volume flow in the great vessels was compared between 2D- and 4D-flow. KE were calculated for all time phases and voxels in the left ventricle.
Results: Phantom results showed high accuracy and precision for both scanners. In vivo, higher accuracy and precision ( P < 0.001) was found for volume flow for the Aera prototype with Resp+ (-3.7 ± 10.4 mL, r = 0.89) compared to the Achieva product sequence (-17.8 ± 18.6 mL, r = 0.56). 4D-flow Resp- on Aera had somewhat larger bias (-9.3 ± 9.6 mL, r = 0.90) compared to Resp+ ( P = 0.005). KE measurements showed larger differences between scanners on the same day compared to the same scanner at different days.
Conclusion: Sequence-specific in vivo validation of 4D-flow is needed before clinical use. 4D-flow with the Aera prototype sequence with a clinically acceptable acquisition time (<10 min) showed acceptable bias in healthy controls to be considered for clinical use. Intra-individual KE comparisons should use the same sequence.
Keywords: 4D-flow; cardiac output; heart failure; valvular regurgitation.
Figures





References
-
- Al-Wakeel N, Fernandes JF, Amiri A, et al. Hemodynamic and energetic aspects of the left ventricle in patients with mitral regurgitation before and after mitral valve surgery. J Magn Reson Imaging 2015; 42: 1705–1712. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
