

Deep brain stimulation in five patients with severe disorders of consciousness
- PMID: 30480031
- PMCID: PMC6243378
- DOI: 10.1002/acn3.648
Deep brain stimulation in five patients with severe disorders of consciousness
Abstract
Objective: The efficacy of deep brain stimulation in disorders of consciousness remains inconclusive. We investigated bilateral 30-Hz low-frequency stimulation designed to overdrive neuronal activity by dual pallido-thalamic targeting, using the Coma Recovery Scale Revised (CRS-R) to assess conscious behavior.
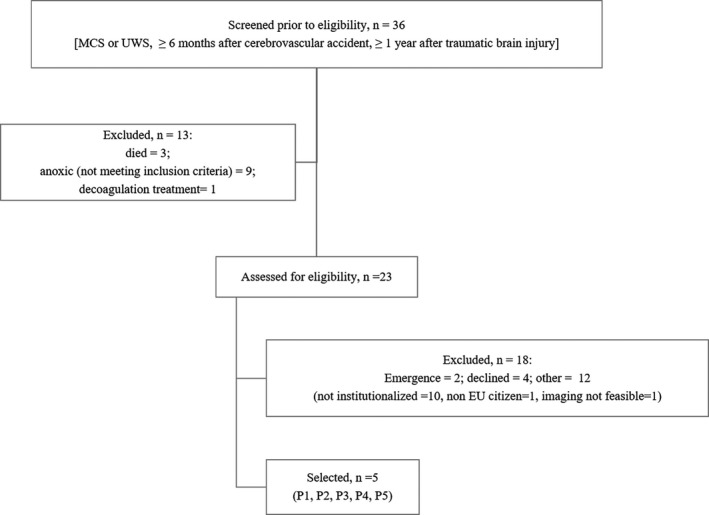
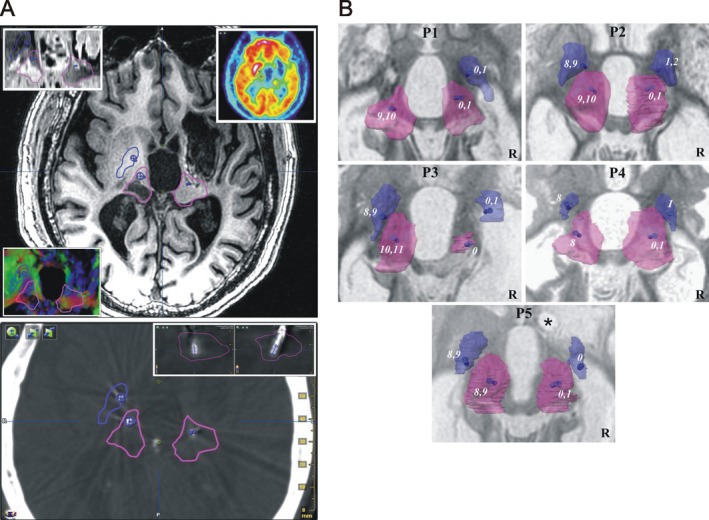
Methods: We conducted a prospective, single center, observational 11-month pilot study comprising four phases: baseline (2 months); surgery and titration (1 month); blind, random, crossover, 1.5-month ON and OFF periods; and unblinded, 5-month stimulation ON. Five adult patients were included: one unresponsive-wakefulness-syndrome male (traumatic brain injury); and four patients in a minimally conscious state, one male (traumatic brain injury) and three females (two hemorrhagic strokes and one traumatic brain injury). Primary outcome measures focused on CRS-R scores. Secondary outcome measures focused notably on baseline brain metabolism and variation in activity (stimulation ON - baseline) using normalized fluorodeoxyglucose positron emission tomography maps. Statistical analysis used random-effect models.
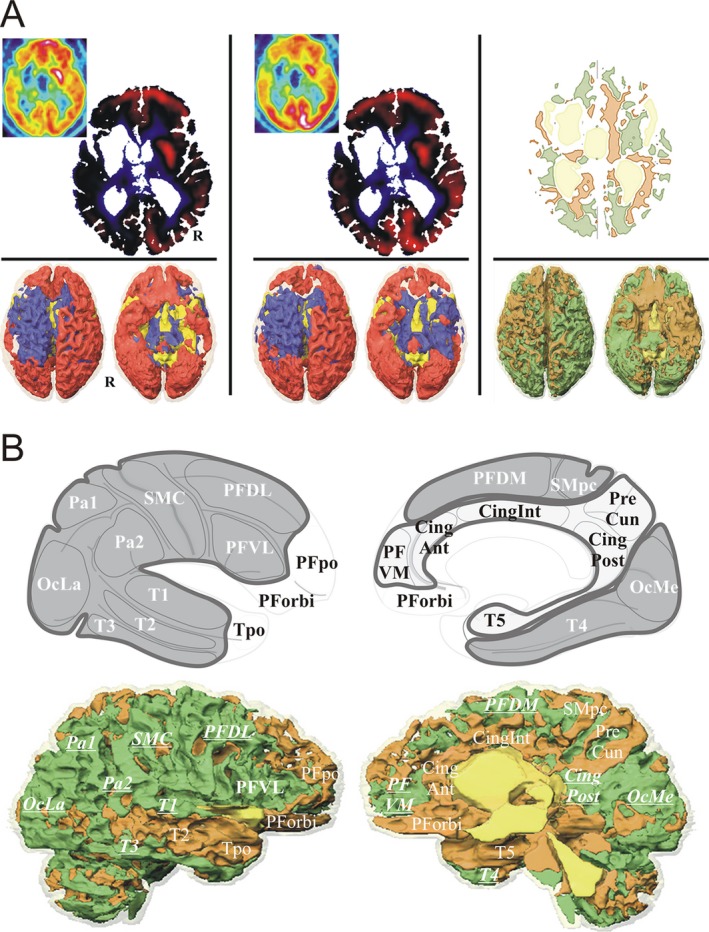
Results: The two male patients (one minimally conscious and one unresponsive wakefulness syndrome) showed improved mean CRS-R scores (stimulation ON vs. baseline), in auditory, visual and oromotor/verbal subscores, and visual subscores respectively. The metabolism of the medial cortices (low at baseline in all five patients) increased specifically in the two responders.
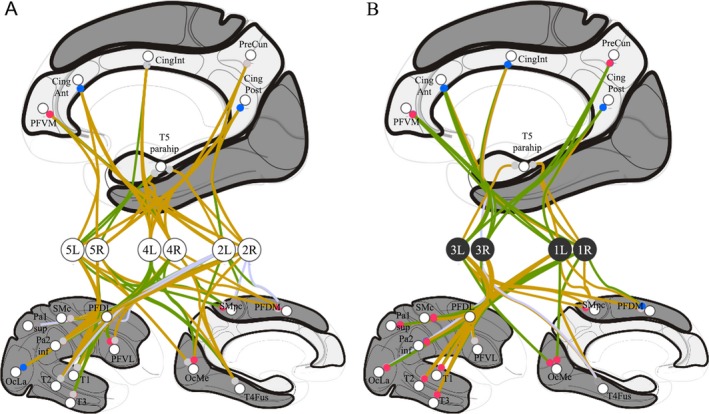
Interpretation: Our findings show there were robust but limited individual clinical benefits, mainly in visual and auditory processes. Overall modifications seem linked to the modulation of thalamo-cortico-basal and tegmental loops activating default mode network cortices. Specifically, in the two responders there was an increase in medial cortex activity related to internal awareness.
Figures
References
-
- Katz DI, Polyak M, Coughlan D, et al. Natural history of recovery from brain injury after prolonged disorders of consciousness: outcome of patients admitted to inpatient rehabilitation with 1‐4 year follow‐up. Prog Brain Res 2009;177:73–88. - PubMed
-
- Ventura T, Harrison‐Felix C, Carlson N, et al. Mortality after discharge from acute care hospitalization with traumatic brain injury: a population‐based study. Arch Phys Med Rehabil 2010;91:20–29. - PubMed
-
- Luauté J, Maucort‐Boulch D, Tell L, et al. Long‐term outcomes of chronic minimally conscious and vegetative states. Neurology 2010;75:246–252. - PubMed
-
- Avesani R, Gambini MG, Albertini G. The vegetative state: a report of two cases with a long‐term follow‐up. Brain Inj 2006;20:333–338. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
