

Regulatory B cells in myasthenia gravis are differentially affected by therapies
- PMID: 30480034
- PMCID: PMC6243377
- DOI: 10.1002/acn3.645
Regulatory B cells in myasthenia gravis are differentially affected by therapies
Abstract
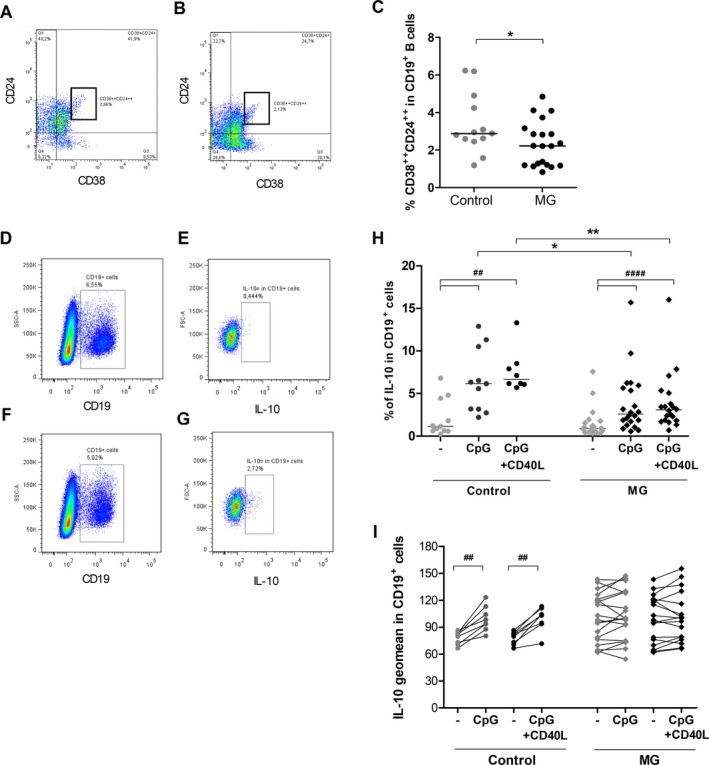
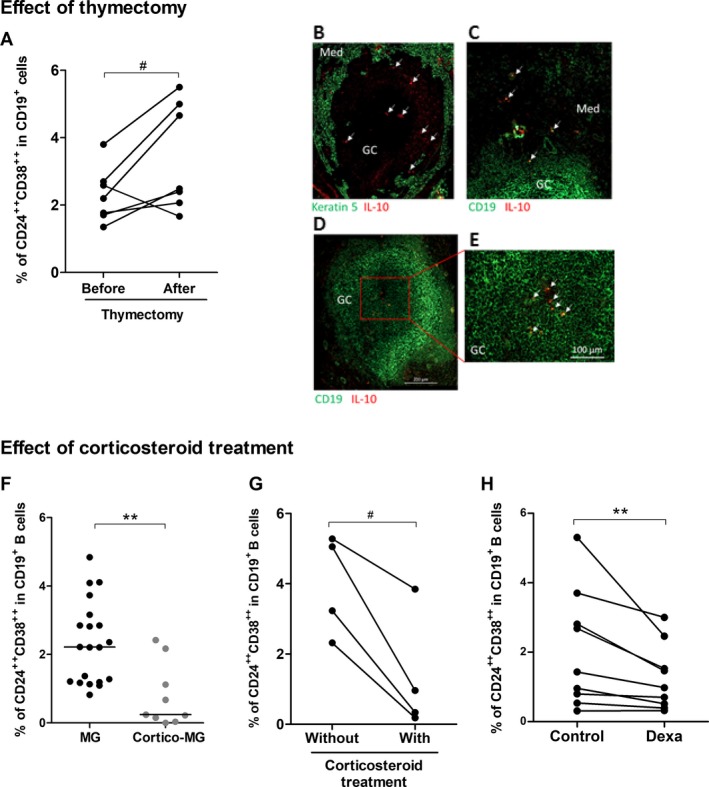
We analyzed the number and functionality of regulatory B (Breg) cells in well-defined myasthenia gravis patients. We first showed a decreased number of circulating CD19+ CD24++ CD38++ Breg cells and an altered functionality of Breg cells in untreated myasthenia gravis patients. Next, we demonstrated that the proportion of circulating Breg cells was restored in myasthenia gravis patients after thymectomy, probably as Breg cells could be sequestered in the myasthenia gravis thymus. In contrast, corticosteroid treatments did not restore and decreased even more the proportion of Breg cells in myasthenia gravis patients. These results clearly demonstrated that two distinct immunomodulatory therapies affect differentially Breg cells.
Figures
References
-
- Berrih‐Aknin S, Le Panse R. Myasthenia gravis: a comprehensive review of immune dysregulation and etiological mechanisms. J Autoimmun 2014;52:90–100. - PubMed
-
- Fillatreau S, Gray D, Anderton SM. Not always the bad guys: B cells as regulators of autoimmune pathology. Nat Rev Immunol 2008;8:391–397. - PubMed
-
- Rosser EC, Mauri C. Regulatory B cells: origin, phenotype, and function. Immunity 2015;42:607–612. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
