

Health Care Costs and Cost-effectiveness in Laryngotracheal Stenosis
- PMID: 30481123
- PMCID: PMC6443425
- DOI: 10.1177/0194599818815068
Health Care Costs and Cost-effectiveness in Laryngotracheal Stenosis
Abstract
Objective: Laryngotracheal stenosis (LTS) is resource-intensive disease. The cost-effectiveness of LTS treatments has not been adequately explored. We aimed to conduct a cost-effectiveness analysis comparing open reconstruction (cricotracheal/tracheal resection [CTR/TR]) with endoscopic dilation in the treatment of LTS.
Study design: Retrospective cohort.
Setting: Tertiary referral center (2013-2017).
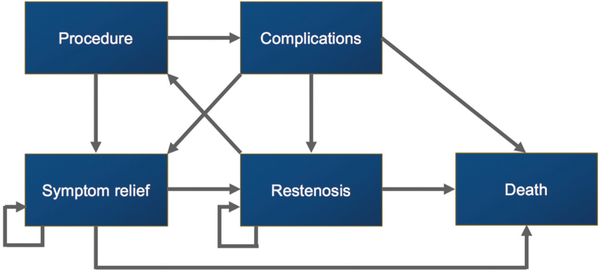
Subjects and methods: Thirty-four LTS patients were recruited. Annual costs were derived from the Department of Otolaryngology-Head and Neck Surgery, Johns Hopkins University. Cost-effectiveness analysis compared CTR/TR versus endoscopic dilation at a willingness-to-pay threshold of $50,000 per quality-adjusted life year (QALY) over 5- and 10-year time horizons. The incremental cost-effectiveness ratio (ICER) was calculated with deterministic analysis and tested for sensitivity with univariate and probabilistic sensitivity analysis.
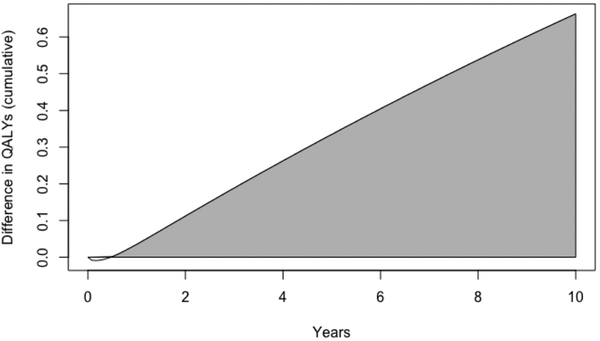
Results: Mean LTS costs were $4080.09 (SE, $569.29) annually for related health care visits. The major risk factor for increased cost was etiology of stenosis. As compared with idiopathic patients, patients with intubation-related stenosis had significantly higher annual costs ($5286.56 vs $2873.62, P = .03). The cost of CTR/TR was $8583.91 (SE, $2263.22). Over a 5-year time horizon, CTR/TR gained $896 per QALY over serial dilations and was cost-effective. Over a 10-year time horizon, CTR/TR dominated dilations with a lower cost and higher QALY.
Conclusion: The cost of treatment for LTS is significant. Patients with intubation-related stenosis have significantly higher annual costs than do idiopathic patients. CTR/TR contributes significantly to cost in LTS but is cost-effective versus endoscopic dilations for appropriately selected patients over a 5- and 10-year horizon.
Keywords: cost; cost-effectiveness; incremental cost-effectiveness ratio; laryngotracheal stenosis; subglottic stenosis.
Conflict of interest statement
Disclosures
Competing interests:
William V. Padula, Monument Analytics—principal, received income; Molnlycke Health Care—Scientific Advisory Board and Speakers Bureau, received income. Zachary Predmore, Analysis Group—salaried position from June to August 2018. Alexander T. Hillel, Olympus USA—consultant.
Figures
References
-
- Rosow DE, Barbarite E. Review of adult laryngotracheal stenosis: pathogenesis, management, and outcomes. Curr Opin Otolaryngol Head Neck Surg. 2016;24:489–493. - PubMed
-
- Hillel AT, Karatayli-Ozgursoy S, Benke JR, et al. Voice quality in laryngotracheal stenosis: impact of dilation and level of stenosis. Ann Otol Rhinol Laryngol. 2015;124:413–418. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
