

Psychological advocacy towards healing (PATH): A randomized controlled trial of a psychological intervention in a domestic violence service setting
- PMID: 30481183
- PMCID: PMC6258512
- DOI: 10.1371/journal.pone.0205485
Psychological advocacy towards healing (PATH): A randomized controlled trial of a psychological intervention in a domestic violence service setting
Abstract
Background: Experience of domestic violence and abuse (DVA) is associated with mental illness. Advocacy has little effect on mental health outcomes of female DVA survivors and there is uncertainty about the effectiveness of psychological interventions for this population.
Objective: To test effectiveness of a psychological intervention delivered by advocates to DVA survivors.
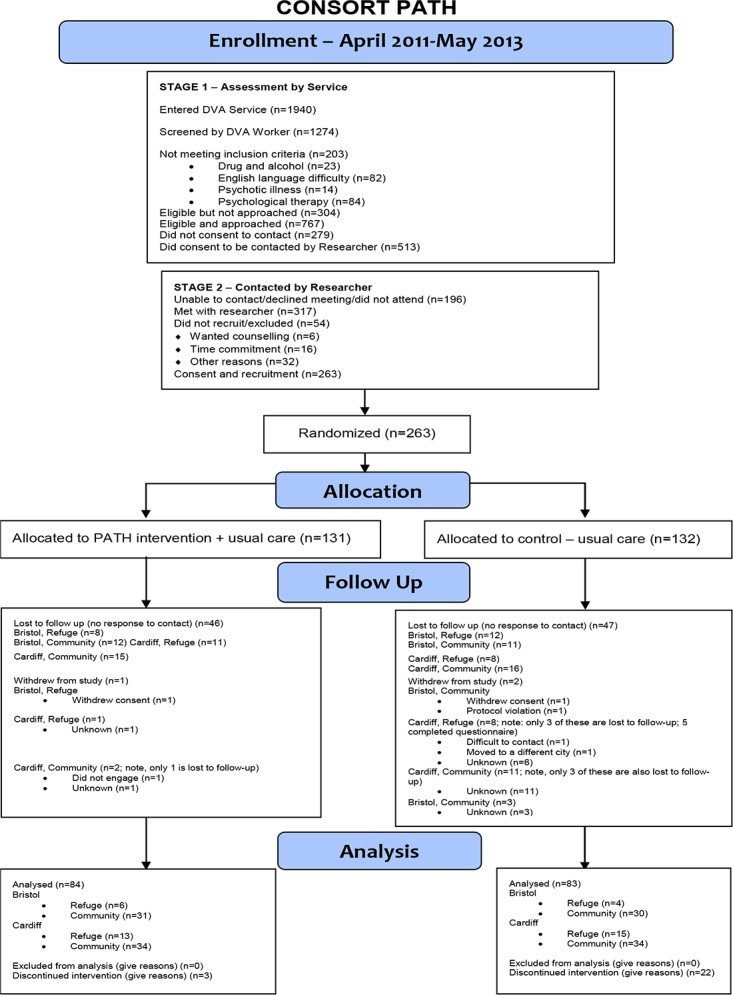
Design, masking, setting, participants: Pragmatic parallel group individually randomized controlled trial of normal DVA advocacy vs. advocacy + psychological intervention. Statistician and researchers blinded to group assignment. Setting: specialist DVA agencies; two UK cities. Participants: Women aged 16 years and older accessing DVA services.
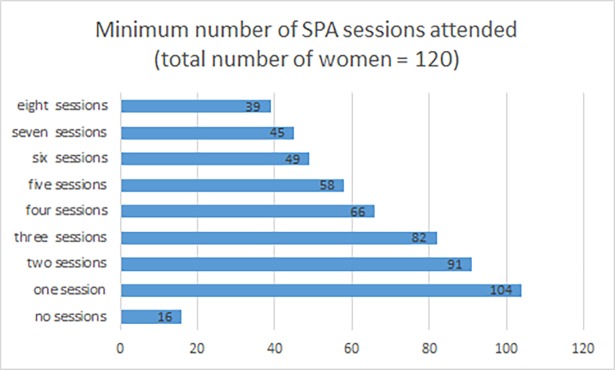
Intervention: Eight specialist psychological advocacy (SPA) sessions with two follow up sessions.
Measurements: Primary outcomes at 12 months: depression symptoms (PHQ-9) and psychological distress (CORE-OM). Primary analysis: intention to treat linear (logistic) regression model for continuous (binary) outcomes.
Results: 263 women recruited (78 in shelter/refuge, 185 in community), 2 withdrew (1 community, control group; 1 intervention, refuge group), 1 was excluded from the study for protocol violation (community, control group), 130 in intervention and 130 in control groups. Recruitment ended June 2013. 12-month follow up: 64%. At 12-month follow up greater improvement in mental health of women in the intervention group. Difference in average CORE-OM score between intervention and control groups: -3.3 points (95% CI -5.5 to -1.2). Difference in average PHQ-9 score between intervention and control group: -2.2 (95% CI -4.1 to -0.3). At 12 months, 35% of the intervention group and 55% of the control group were above the CORE-OM -2clinical threshold (OR 0.32, 95% CI 0.16 to 0.64); 29% of the intervention group and 46% of the control group were above the PHQ-9 clinical threshold (OR 0.41, 95% CI 0.21 to 0.81).
Limitations: 64% retention at 12 months.
Conclusions: An eight-session psychological intervention delivered by DVA advocates produced clinically relevant improvement in mental health outcomes compared with normal advocacy care.
Trial registration: ISRCTN registry ISRCTN58561170 Original Research 3675/3750.
Conflict of interest statement
The authors of this manuscript have the following competing interests: If the PATH intervention was implemented in service settings, Davies would receive payment for training and supervising specialist psychological advocates. Domestic Violence Training Ltd provided support in the form of salary to author AD.
Figures
References
-
- WHO. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence Geneva: WHO; 2013.
-
- Trevillion K, Oram S, Feder G, Howard LM. Experiences of Domestic Violence and Mental Disorders: A Systematic Review and Meta-Analysis. PLoS ONE. 2012;7(12):e51740 10.1371/journal.pone.0051740 - DOI - PMC - PubMed
-
- Devries KM, Mak JYT, García-Moreno C, Petzold M, Child JC, Falder G, et al. The Global Prevalence of Intimate Partner Violence Against Women. Science. 2013;340(6140):1527–8. 10.1126/science.1240937 - DOI - PubMed
-
- Ramsay J, Feder G, Rivas C. Interventions to reduce violence and promote the physical and psychosocial well-being of women who experience partner abuse: a systematic review. In: Health Do, editor. London2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
