

Enhancing the prediction of acute kidney injury risk after percutaneous coronary intervention using machine learning techniques: A retrospective cohort study
- PMID: 30481186
- PMCID: PMC6258473
- DOI: 10.1371/journal.pmed.1002703
Enhancing the prediction of acute kidney injury risk after percutaneous coronary intervention using machine learning techniques: A retrospective cohort study
Abstract
Background: The current acute kidney injury (AKI) risk prediction model for patients undergoing percutaneous coronary intervention (PCI) from the American College of Cardiology (ACC) National Cardiovascular Data Registry (NCDR) employed regression techniques. This study aimed to evaluate whether models using machine learning techniques could significantly improve AKI risk prediction after PCI.
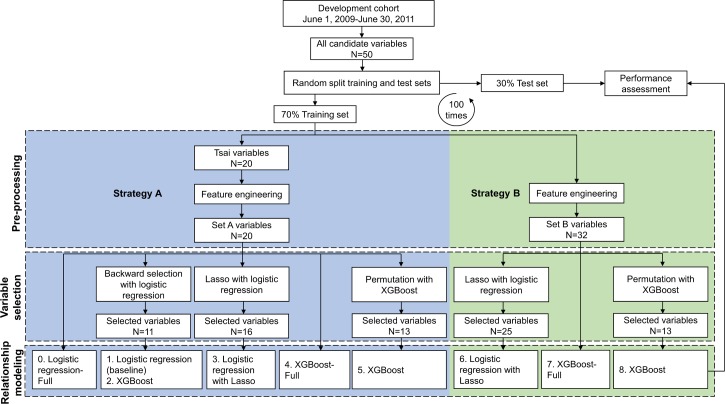
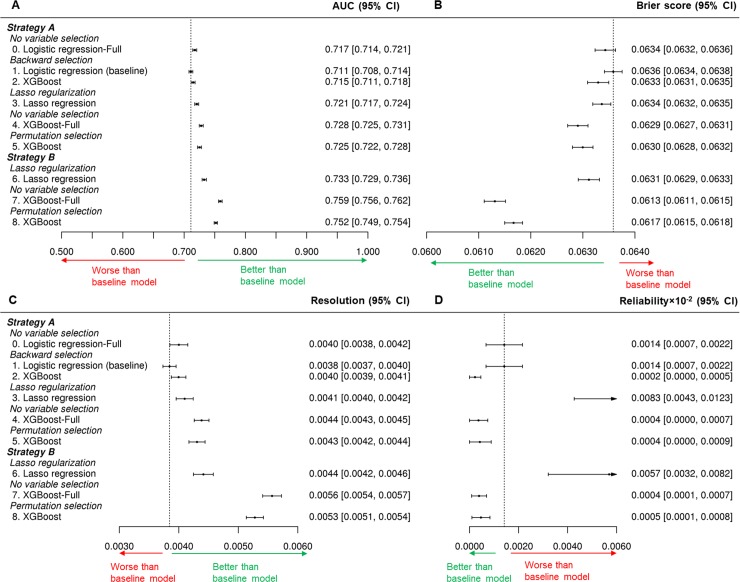
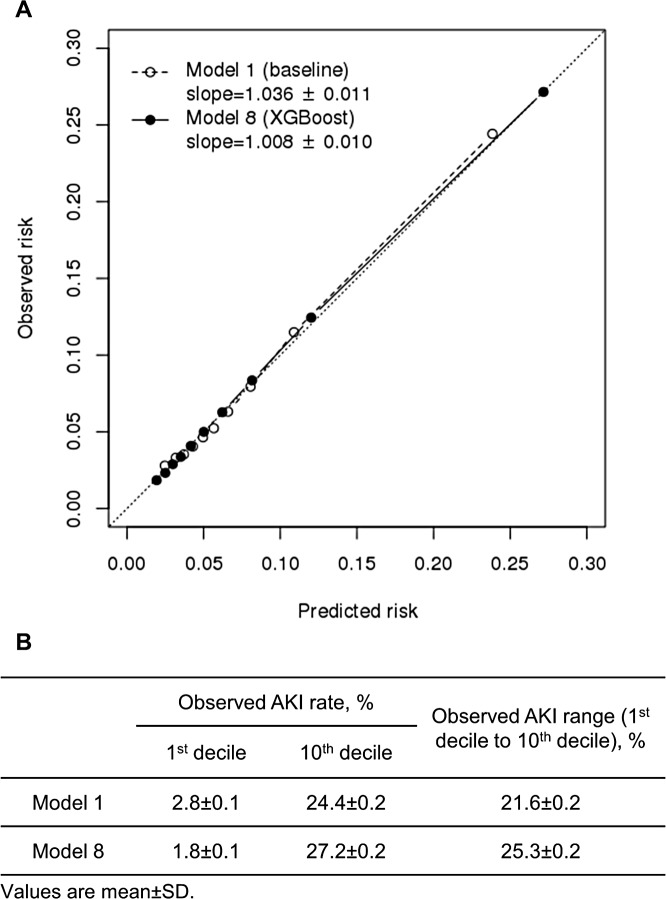
Methods and findings: We used the same cohort and candidate variables used to develop the current NCDR CathPCI Registry AKI model, including 947,091 patients who underwent PCI procedures between June 1, 2009, and June 30, 2011. The mean age of these patients was 64.8 years, and 32.8% were women, with a total of 69,826 (7.4%) AKI events. We replicated the current AKI model as the baseline model and compared it with a series of new models. Temporal validation was performed using data from 970,869 patients undergoing PCIs between July 1, 2016, and March 31, 2017, with a mean age of 65.7 years; 31.9% were women, and 72,954 (7.5%) had AKI events. Each model was derived by implementing one of two strategies for preprocessing candidate variables (preselecting and transforming candidate variables or using all candidate variables in their original forms), one of three variable-selection methods (stepwise backward selection, lasso regularization, or permutation-based selection), and one of two methods to model the relationship between variables and outcome (logistic regression or gradient descent boosting). The cohort was divided into different training (70%) and test (30%) sets using 100 different random splits, and the performance of the models was evaluated internally in the test sets. The best model, according to the internal evaluation, was derived by using all available candidate variables in their original form, permutation-based variable selection, and gradient descent boosting. Compared with the baseline model that uses 11 variables, the best model used 13 variables and achieved a significantly better area under the receiver operating characteristic curve (AUC) of 0.752 (95% confidence interval [CI] 0.749-0.754) versus 0.711 (95% CI 0.708-0.714), a significantly better Brier score of 0.0617 (95% CI 0.0615-0.0618) versus 0.0636 (95% CI 0.0634-0.0638), and a better calibration slope of observed versus predicted rate of 1.008 (95% CI 0.988-1.028) versus 1.036 (95% CI 1.015-1.056). The best model also had a significantly wider predictive range (25.3% versus 21.6%, p < 0.001) and was more accurate in stratifying AKI risk for patients. Evaluated on a more contemporary CathPCI cohort (July 1, 2015-March 31, 2017), the best model consistently achieved significantly better performance than the baseline model in AUC (0.785 versus 0.753), Brier score (0.0610 versus 0.0627), calibration slope (1.003 versus 1.062), and predictive range (29.4% versus 26.2%). The current study does not address implementation for risk calculation at the point of care, and potential challenges include the availability and accessibility of the predictors.
Conclusions: Machine learning techniques and data-driven approaches resulted in improved prediction of AKI risk after PCI. The results support the potential of these techniques for improving risk prediction models and identification of patients who may benefit from risk-mitigation strategies.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: SSD is supported by the Department of Veterans Affairs. WLS is a consultant for Hugo, a personal health information platform. CIM is a consultant for Cook, Bard, Medtronic, Abbott and Cardinal Health. FPW is supported by the National Science Foundation grant R01DK113191. JSR is the Chief Innovation Officer for the American College of Cardiology. HMK is a recipient of research agreements from Medtronic and from Johnson & Johnson (Janssen), through Yale University, to develop methods of clinical trial data sharing; was the recipient of a grant from the Food and Drug Administration and Medtronic to develop methods for postmarket surveillance of medical devices; works under contract with the Centers for Medicare and Medicaid Services to develop and maintain performance measures; chairs a cardiac scientific advisory board for UnitedHealth; is a member of the Advisory Board for Element Science and the Physician Advisory Board for Aetna; is a participant/participant representative of the IBM Watson Health Life Sciences Board; and is the founder of Hugo, a personal health information platform. JAS is supported by grants from Gilead, Genentech, Lilly, Amorcyte, and EvaHeart and has a patent for the Seattle Angina Questionnaire with royalties paid. He also owns the copyright to the Seattle Angina Questionnaire. He is the PI of an Analytic Center for the American College of Cardiology Foundation and has an equity interest in Health Outcomes Sciences. FAM has a contract (through his primary institution) for his role as Chief Science Officer of the NCDR. BJM is an associate editor for PLOS ONE, which is involved in this special issue. He has a relationship with the American College of Cardiology in selecting and pursuing innovative research based upon their registry data (unrelated to this paper). He has a pending patent application for an EHR-based prediction tool in Yale New Haven Health, as well as two funded studies, one by the DoD-Advanced Research Projects Agency and one with the NSF to support student travel to conferences in the body sensor networks field. American College of Cardiology may incorporate this work, or future iterations, into its registry. No other organisation named above has a competing interest in relation to this work. The other authors report no potential competing interests.
Figures
References
-
- Bartholomew BA, Harjai KJ, Dukkipati S, Boura JA, Yerkey MW, Glazier S, et al. Impact of nephropathy after percutaneous coronary intervention and a method for risk stratification. Am J Cardiol. 2004;93(12):1515–9. Epub 2004/06/15. 10.1016/j.amjcard.2004.03.008 - DOI - PubMed
-
- Brown JR, DeVries JT, Piper WD, Robb JF, Hearne MJ, Ver Lee PM, et al. Serious renal dysfunction after percutaneous coronary interventions can be predicted. Am Heart J. 2008;155(2):260–6. Epub 2008/01/25. 10.1016/j.ahj.2007.10.007 - DOI - PubMed
-
- Mueller C, Buerkle G, Buettner HJ, Petersen J, Perruchoud AP, Eriksson U, et al. Prevention of contrast media-associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty. Arch Intern Med. 2002;162(3):329–36. - PubMed
-
- Meier P, Ko DT, Tamura A, Tamhane U, Gurm HS. Sodium bicarbonate-based hydration prevents contrast-induced nephropathy: a meta-analysis. BMC Med. 2009;7:23 10.1186/1741-7015-7-23 - DOI - PMC - PubMed
-
- Brown JR, Robb JF, Block CA, Schoolwerth AC, Kaplan AV, O'Connor GT, et al. Does safe dosing of iodinated contrast prevent contrast-induced acute kidney injury? Circ Cardiovasc Interv. 2010;3(4):346–50. 10.1161/CIRCINTERVENTIONS.109.910638 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
