

Treating chronic insomnia in postmenopausal women: a randomized clinical trial comparing cognitive-behavioral therapy for insomnia, sleep restriction therapy, and sleep hygiene education
- PMID: 30481333
- PMCID: PMC6369725
- DOI: 10.1093/sleep/zsy217
Treating chronic insomnia in postmenopausal women: a randomized clinical trial comparing cognitive-behavioral therapy for insomnia, sleep restriction therapy, and sleep hygiene education
Abstract
Study objectives: Insomnia is a leading cause of disability in postmenopausal women. Multicomponent cognitive-behavioral therapy for insomnia (CBTI) is a first-line treatment for chronic insomnia, but support for its efficacy in treating menopause-related insomnia is scarce. The present study evaluated whether CBTI is an efficacious treatment for menopause-related chronic insomnia, and whether sleep restriction therapy (SRT)-a single component of CBTI-is equally efficacious compared with CBTI.
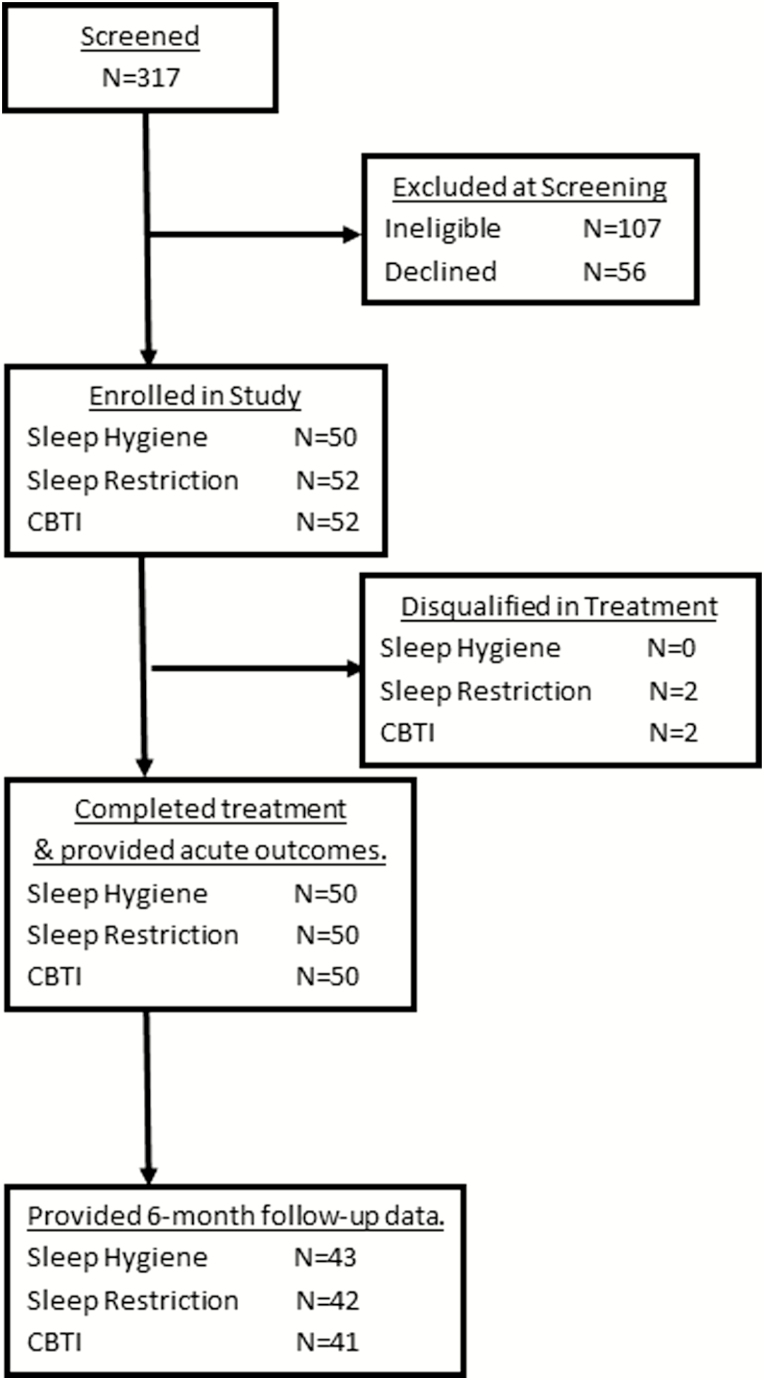
Methods: In a single-site, randomized controlled trial, 150 postmenopausal women (56.44 ± 5.64 years) with chronic DSM-5 insomnia disorder related to menopause were randomized to three treatment conditions: sleep hygiene education (SHE), SRT, or CBTI. Blinded assessments were performed at baseline, posttreatment, and 6 months after treatment. The Insomnia Severity Index (ISI) and sleep diaries served as primary outcomes.
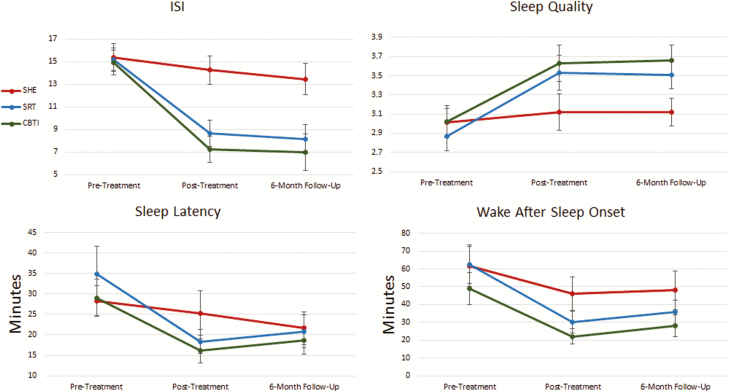
Results: From baseline to posttreatment, ISI decreased 7.70 points in the CBTI group (p < .001), 6.56 points in the SRT group (p < .001), and 1.12 in the SHE group (p = .01). Although average sleep duration increased in all groups by 6 month follow-up, CBTI patients obtained 40-43 more minutes of nightly sleep than those who received SHE or SRT. Remission rates in the CBTI (54%-84%) and SRT (38%-57%) groups were higher than SHE patients (4%-33%) at posttreatment and 6 month follow-up. CBTI patients were generally more likely to remit than SRT patients.
Conclusions: CBTI and SRT effectively treat menopause-related insomnia disorder and are superior to SHE. Response to CBTI and SRT is similar, but CBTI outperforms SRT in improving sleep maintenance, which may increase likelihood of remission. Clinical Trial Name: Behavioral Treatment of Menopausal Insomnia: Sleep and Daytime Outcomes. URL: clinicaltrials.gov. Registration: NCT01933295.
Figures
References
-
- Kravitz HM, et al. . Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause. 2003;10(1):19–28. - PubMed
-
- Eichling PS, et al. . Menopause related sleep disorders. J Clin Sleep Med. 2005;1(3):291–300. - PubMed
-
- Attarian H, et al. . Treatment of chronic insomnia disorder in menopause: evaluation of literature. Menopause. 2015;22(6):674–684. - PubMed
-
- Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6(2):97–111. - PubMed
