

Do Out-of-Hospital Cardiac Arrest Patients Have Increased Chances of Survival When Transported to a Cardiac Resuscitation Center?
- PMID: 30482128
- PMCID: PMC6405559
- DOI: 10.1161/JAHA.118.011079
Do Out-of-Hospital Cardiac Arrest Patients Have Increased Chances of Survival When Transported to a Cardiac Resuscitation Center?
Abstract
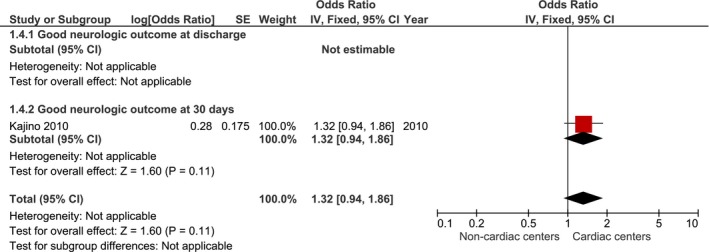
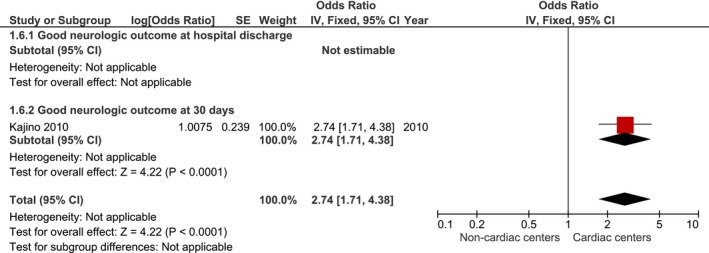
Background Patients suffering from an out-of-hospital cardiac arrest are often transported to the closest hospital. Although it has been suggested that these patients be transported to cardiac resuscitation centers, few jurisdictions have acted on this recommendation. To better evaluate the evidence on this subject, a systematic review and meta-analysis of the currently available literature evaluating the association between the destination hospital's capability (cardiac resuscitation center or not) and resuscitation outcomes for adult patients suffering from an out-of-hospital cardiac arrest was performed. Methods and Results PubMed, EMBASE , and the Cochrane Library databases were first searched using a specifically designed search strategy. Both original randomized controlled trials and observational studies were considered for inclusion. Cardiac resuscitation centers were defined as having on-site percutaneous coronary intervention and targeted temperature management capability at all times. The primary outcome measure was survival. Twelve nonrandomized observational studies were retained in this review. A total of 61 240 patients were included in the 10 studies that could be included in the meta-analysis regarding the survival outcome. Being transported to a cardiac resuscitation center was associated with an increase in survival (odds ratio=1.95 [95% confidence interval 1.47-2.59], P<0.001). Conclusions Adult patients suffering from an out-of-hospital cardiac arrest transported to cardiac resuscitation centers have better outcomes than their counterparts. When possible, it is reasonable to transport these patients directly to cardiac resuscitation centers (class II a, level of evidence B, nonrandomized). Clinical Trial Registration URL : www.crd.york.ac.uk/PROSPERO/ . Unique identifier: CRD 42018086608.
Keywords: cardiac arrest; emergency medical services; percutaneous coronary intervention; resuscitation; sudden cardiac arrest.
Figures
















Similar articles
-
Direct Transport to a Percutaneous Cardiac Intervention Center and Outcomes in Patients With Out-of-Hospital Cardiac Arrest.Circ Cardiovasc Qual Outcomes. 2017 Jun;10(6):e003414. doi: 10.1161/CIRCOUTCOMES.116.003414. Circ Cardiovasc Qual Outcomes. 2017. PMID: 28615177
-
Direct transport to PCI-capable hospitals after out-of-hospital cardiac arrest in New Zealand: Inequities and outcomes.Resuscitation. 2019 Sep;142:111-116. doi: 10.1016/j.resuscitation.2019.06.283. Epub 2019 Jul 2. Resuscitation. 2019. PMID: 31271727
-
Direct transport to a PCI-capable hospital is associated with improved survival after adult out-of-hospital cardiac arrest of medical aetiology.Resuscitation. 2018 Jul;128:76-82. doi: 10.1016/j.resuscitation.2018.04.039. Epub 2018 May 2. Resuscitation. 2018. PMID: 29729284
-
Chest-compression-only versus conventional cardiopulmonary resuscitation by bystanders for children with out-of-hospital cardiac arrest: A systematic review and meta-analysis.Resuscitation. 2019 Jan;134:81-90. doi: 10.1016/j.resuscitation.2018.10.032. Epub 2018 Nov 2. Resuscitation. 2019. PMID: 30391520
-
Manual Cardiopulmonary Resuscitation Versus CPR Including a Mechanical Chest Compression Device in Out-of-Hospital Cardiac Arrest: A Comprehensive Meta-analysis From Randomized and Observational Studies.Ann Emerg Med. 2016 Mar;67(3):349-360.e3. doi: 10.1016/j.annemergmed.2015.09.023. Epub 2015 Nov 19. Ann Emerg Med. 2016. PMID: 26607332 Review.
Cited by
-
Impact of Transport Time and Cardiac Arrest Centers on the Neurological Outcome After Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Study.J Am Heart Assoc. 2020 Jun 2;9(11):e015544. doi: 10.1161/JAHA.119.015544. Epub 2020 May 27. J Am Heart Assoc. 2020. PMID: 32458720 Free PMC article.
-
Association between direct transport to a cardiac arrest centre and survival following out-of-hospital cardiac arrest: A propensity-matched Aotearoa New Zealand study.Resusc Plus. 2024 Apr 6;18:100625. doi: 10.1016/j.resplu.2024.100625. eCollection 2024 Jun. Resusc Plus. 2024. PMID: 38601710 Free PMC article.
-
Direct Transport to Cardiac Arrest Center and Survival Outcomes after Out-of-Hospital Cardiac Arrest by Urbanization Level.J Clin Med. 2022 Feb 16;11(4):1033. doi: 10.3390/jcm11041033. J Clin Med. 2022. PMID: 35207304 Free PMC article.
-
Postarrest Interventions that Save Lives.Emerg Med Clin North Am. 2020 Nov;38(4):771-782. doi: 10.1016/j.emc.2020.06.001. Epub 2020 Jul 21. Emerg Med Clin North Am. 2020. PMID: 32981616 Free PMC article. Review.
-
Impact of Cardiac Arrest Centers on the Survival of Patients With Nontraumatic Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2022 Jan 4;11(1):e023806. doi: 10.1161/JAHA.121.023806. Epub 2021 Dec 20. J Am Heart Assoc. 2022. PMID: 34927456 Free PMC article.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER III, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–e322. - PubMed
-
- Weisfeldt ML, Sitlani CM, Ornato JP, Rea T, Aufderheide TP, Davis D, Dreyer J, Hess EP, Jui J, Maloney J, Sopko G, Powell J, Nichol G, Morrison LJ; ROC Investigators . Survival after application of automatic external defibrillators before arrival of the emergency medical system: evaluation in the Resuscitation Outcomes Consortium population of 21 million. J Am Coll Cardiol. 2010;55:1713–1720. - PMC - PubMed
-
- Perkins GD, Cooke MW. Variability in cardiac arrest survival: the NHS Ambulance Service Quality Indicators. Emerg Med J. 2012;29:3–5. - PubMed
-
- Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out‐of‐hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81:1479–1487. - PubMed
-
- Kronick SL, Kurz MC, Lin S, Edelson DP, Berg RA, Billi JE, Cabanas JG, Cone DC, Diercks DB, Foster JJ, Meeks RA, Travers AH, Welsford M. Part 4: systems of care and continuous quality improvement: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S397–S413. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
