

Comparison of non-invasive to invasive oxygenation ratios for diagnosing acute respiratory distress syndrome following coronary artery bypass graft surgery: a prospective derivation-validation cohort study
- PMID: 30482210
- PMCID: PMC6260696
- DOI: 10.1186/s13019-018-0804-8
Comparison of non-invasive to invasive oxygenation ratios for diagnosing acute respiratory distress syndrome following coronary artery bypass graft surgery: a prospective derivation-validation cohort study
Abstract
Objective: To determine if non-invasive oxygenation indices, namely peripheral capillary oxygen saturation (SpO2)/fraction of inspired oxygen (FiO2) and partial pressure of alveolar oxygen (PAO2)/FiO2 may be used as effective surrogates for the partial pressure of arterial oxygen (PaO2)/FiO2. Also, to determine the SpO2/FiO2 and PAO2/FiO2 values that correspond to PaO2/FiO2 thresholds for identifying acute respiratory distress syndrome (ARDS) in patients following coronary artery bypass graft (CABG) surgery.
Methods: A prospective derivation-validation cohort study in the Open-Heart ICU of an academic teaching hospital. Recorded variables included patient demographics, ventilator settings, chest radiograph results, and SPO2, PaO2, PAO2, SaO2, and FiO2. Linear regression modeling was used to quantify the relationship between indices. Receiver operating characteristic (ROC) curves were used to determine the sensitivity and specificity of the threshold values.
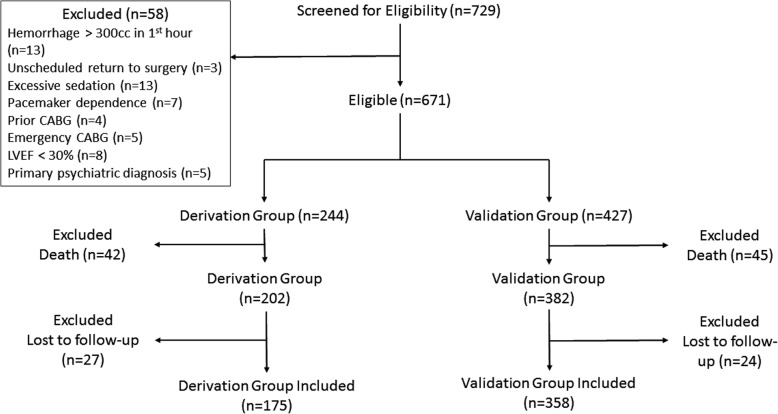
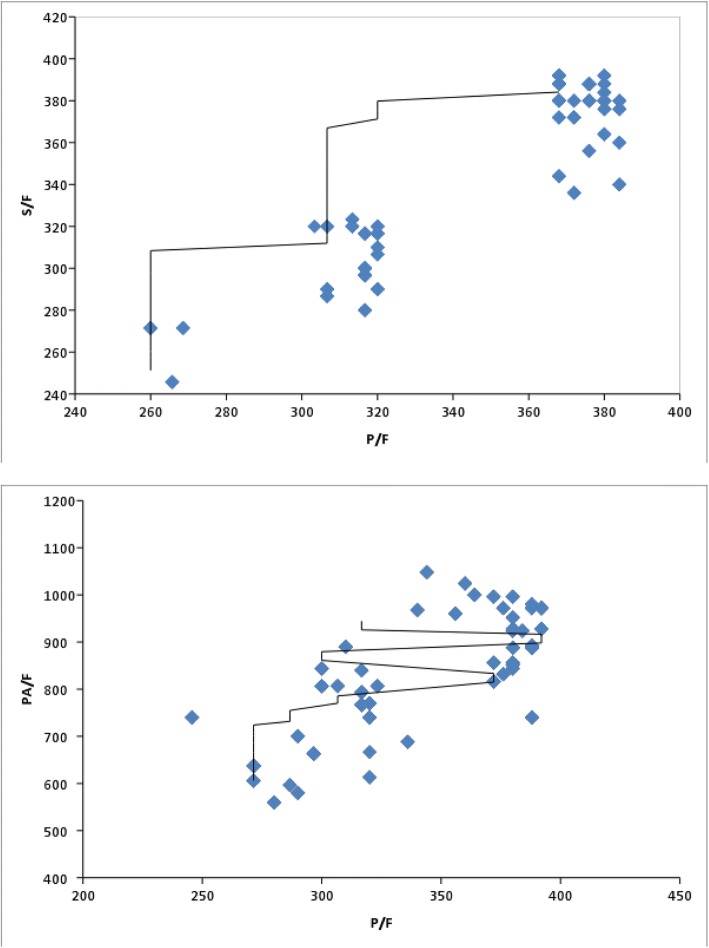
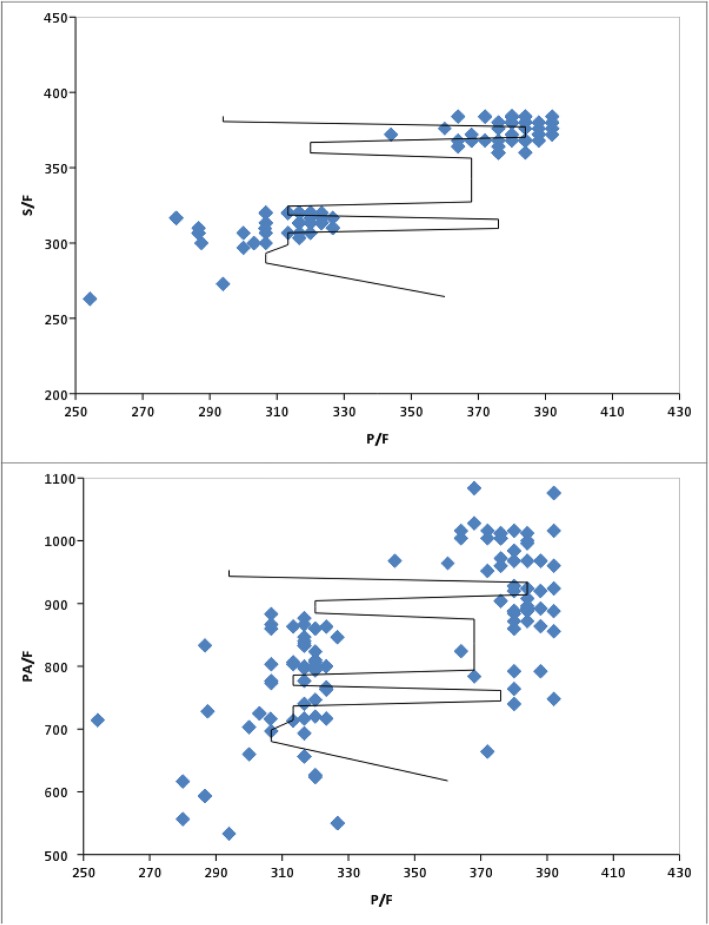
Results: One-hundred seventy-five patients were enrolled in the derivation cohort, and 358 in the validation cohort. The SPO2/FiO2 and PAO2/FiO2 ratios could be predicted well from PaO2/FiO2, described by the linear regression models SPO2/FiO2 = 71.149 + 0.8PF and PAO2/FiO2 = 38.098 + 2.312PF, respectively. According to the linear regression equation, a PaO2/FiO2 ratio of 300 equaled an SPO2/FiO2 ratio of 311 (R2 0.857, F 1035.742, < 0.0001) and a PAO2/FiO2 ratio of 732 (R2 0.576, F 234.887, < 0.0001). The SPO2/FiO2 threshold of 311 had 90% sensitivity, 80% specificity, LR+ 4.50, LR- 0.13, PPV 98, and NPV 42.1 for the diagnosis of mild ARDS. The PAO2/FiO2 threshold of 732 had 86% sensitivity, 90% specificity, LR+ 8.45, LR- 0.16, PPV 98.9, and NPV 36 for the diagnosis of mild ARDS. SPO2/FiO2 had excellent discrimination ability for mild ARDS (AUC ± SE = 0.92 ± 0.017; 95% CI 0.889 to 0.947) as did PAO2/FiO2 (AUC ± SE = 0.915 ± 0.018; 95% CI 0.881 to0.942).
Conclusions: PaO2 and SaO2 correlated in the diagnosis of ARDS, with a PaO2/FiO2 of 300 correlating to an SPO2/ FiO2 of 311 (Sensitivity 90%, Specificity 80%). The SPO2/ FiO2 ratio may allow for early real-time rapid identification of ARDS, while decreasing the cost, phlebotomy, blood loss, pain, skin breaks, and vascular punctures associated with serial arterial blood gas measurements.
Keywords: Acute respiratory distress syndrome; Coronary artery bypass graft surgery; Oxygenation indices; Ratio of arterial oxygen partial pressure to fractional inspired oxygen; Ratio of partial pressure of alveolar oxygen to fractional inspired oxygen; Ratio of peripheral capillary oxygen saturation to fractional inspired oxygen.
Conflict of interest statement
Author’s information
Dr. Miller is residency trained in both Emergency Medicine and Internal Medicine from the State University of New York (SUNY) Downstate Medical Center in Brooklyn, NY. He then completed fellowships in Pulmonary Medicine at the University of Pittsburgh Medical Center in Pittsburgh, PA, followed by Critical Care Medicine at the National Institutes of Health in Bethesda, MD. He is currently Clinical Associate Professor and Chief, Division of Research in the Department of Emergency Medicine at East Carolina University Brody School of Medicine. He is highly published and experienced in the clinical investigation of respiratory failure, resuscitation, and shock. Dr. Miller is Director of the MORZAK Collaborative through which he has cultivated a strong working relationship with investigators in numerous countries. In the current project, Dr. Miller worked with investigators in Iran to investigate whether non-invasive oxygenation indicies may be used to diagnose ARDS in post-op patient’s following CABG surgery.
Ethics approval and consent to participate
The protocol was approved by the investigational review board at Baqiyatallah University of Medical Sciences. Consent was required and covered both study participation and publication of findings. Informed consent was required prior to cardiac arrest event and could be provided by the patient, legal guardian, or healthcare surrogate.
Consent for publication
The informed consent included permission to present and publish de-identified results.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Vahedian-Azimi A, Sadeghi M, Movafegh A, Zanjani RS, Hasani D, Salehmoghaddam A, et al. The relationship between perceived stress and the top five heart disease characteristics in patients with myocardial infarction. J Zanjan Univ Med Sci. 2012;20(78):100–112.
-
- Laslett LJ, Alagona P, Clark BA, Drozda JP, Saldivar F, Wilson SR, et al. The worldwide environment of cardiovascular disease: prevalence, diagnosis, therapy, and policy issues: a report from the American College of Cardiology. J Am Coll Cardiol. 2012;60(25 Suppl):1. doi: 10.1016/j.jacc.2012.11.002. - DOI - PubMed
-
- Naghavi M, Wang H, Lozano R, Davis A, Liang X, Zhou M, et al. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–171. doi: 10.1016/S0140-6736(14)61682-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
