

A systematic review and meta-analysis of stereotactic body radiation therapy versus surgery for patients with non-small cell lung cancer
- PMID: 30482524
- PMCID: PMC6582640
- DOI: 10.1016/j.jtcvs.2018.08.075
A systematic review and meta-analysis of stereotactic body radiation therapy versus surgery for patients with non-small cell lung cancer
Abstract
Objective: Stereotactic body radiation therapy is the preferred treatment modality for patients with inoperable early-stage non-small cell lung cancer. However, comparative outcomes between stereotactic body radiation therapy and surgery for high-risk patients remain controversial. The primary aim of the present meta-analysis was to assess overall survival in matched and unmatched patient cohorts undergoing stereotactic body radiation therapy or surgery. Secondary end points included cancer-specific survival, disease-free survival, disease recurrence, and perioperative outcomes.
Methods: A systematic review of relevant studies was performed through online databases using predefined criteria. The most updated studies were selected for meta-analysis according to unmatched and matched patient cohorts.
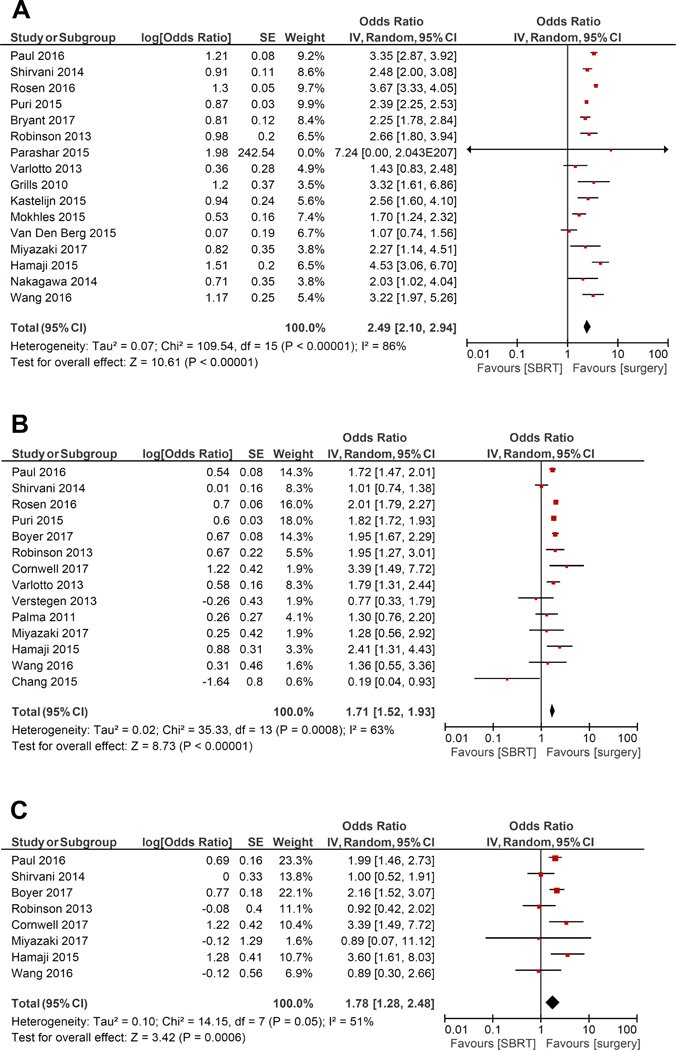
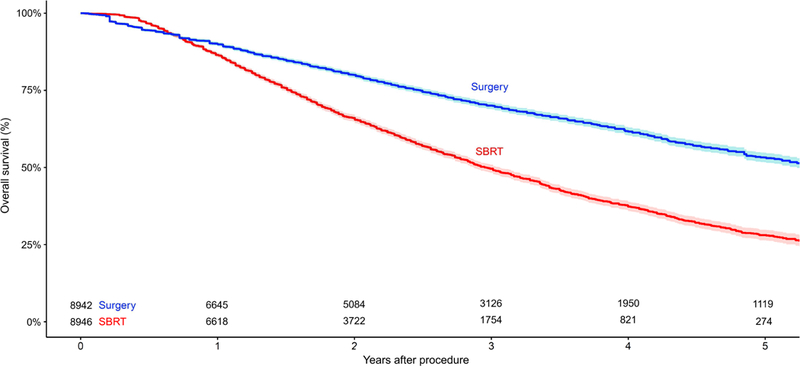
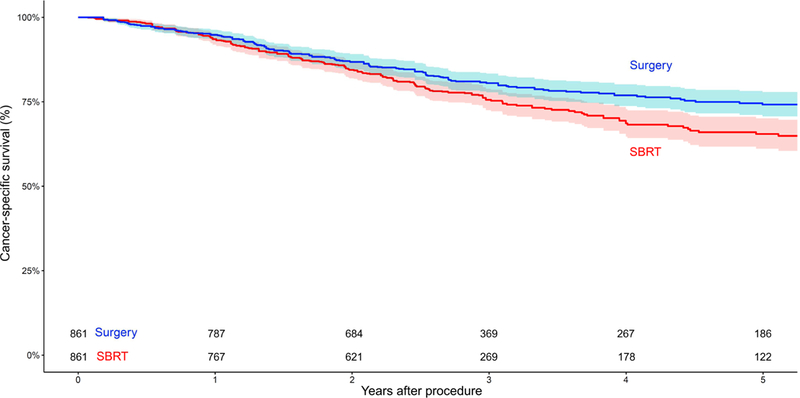
Results: Thirty-two studies were identified in the systematic review, and 23 were selected for quantitative analysis. Surgery was associated with superior overall survival in both unmatched (odds ratio, 2.49; 95% confidence interval, 2.10-2.94; P < .00001) and matched (odds ratio, 1.71; 95% confidence interval, 1.52-1.93; P < .00001) cohorts. Subgroup analysis demonstrated superior overall survival for lobectomy and sublobar resection compared with stereotactic body radiation therapy. In unmatched and matched cohorts, cancer-specific survival, disease-free survival, and freedom from locoregional recurrence were superior after surgery. However, stereotactic body radiation therapy was associated with fewer perioperative deaths.
Conclusions: The current evidence suggests surgery is superior to stereotactic body radiation therapy in terms of mid- and long-term clinical outcomes; stereotactic body radiation therapy is associated with lower perioperative mortality. However, the improved outcomes after surgery may be due at least in part to an imbalance of baseline characteristics. Future studies should aim to provide histopathologic confirmation of malignancy and compare stereotactic body radiation therapy with minimally invasive anatomical resections.
Keywords: meta-analysis; non–small cell lung cancer; stereotactic body radiation therapy; surgery; survival.
Copyright © 2018 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
COI Statement:
A.R. has received funding from Varian Medical Systems, Boehringer Ingelheim, Pfizer, and Astra Zeneca. All other authors have no potential conflicts of interest.
Figures
Comment in
-
Surgery versus stereotactic body radiation therapy: Definitive evidence is still elusive.J Thorac Cardiovasc Surg. 2019 Jan;157(1):374-375. doi: 10.1016/j.jtcvs.2018.10.012. Epub 2018 Oct 14. J Thorac Cardiovasc Surg. 2019. PMID: 30557954 No abstract available.
-
Stereotactic body radiation therapy versus surgery for early stage non-small cell lung cancer: clearing a path through an evolving treatment landscape.J Thorac Dis. 2019 May;11(Suppl 9):S1360-S1365. doi: 10.21037/jtd.2019.03.91. J Thorac Dis. 2019. PMID: 31245133 Free PMC article. No abstract available.
-
Substantial imbalance that is never eliminated with propensity score matched analyses in comparing surgery to stereotactic body radiotherapy for patients with early-stage non-small cell lung cancer.J Thorac Dis. 2019 May;11(Suppl 9):S1415-S1419. doi: 10.21037/jtd.2019.03.11. J Thorac Dis. 2019. PMID: 31245148 Free PMC article. No abstract available.
-
Verification of meta-analysis and propensity-matched analysis comparing stereotactic body radiation therapy versus surgery for early stage lung cancer.J Thorac Dis. 2019 Jun;11(6):2201-2204. doi: 10.21037/jtd.2019.06.06. J Thorac Dis. 2019. PMID: 31372252 Free PMC article. No abstract available.
Similar articles
-
Stereotactic body radiation therapy versus surgical resection for stage I non-small cell lung cancer.J Thorac Cardiovasc Surg. 2010 Aug;140(2):377-86. doi: 10.1016/j.jtcvs.2009.12.054. Epub 2010 Apr 18. J Thorac Cardiovasc Surg. 2010. PMID: 20400121
-
A national analysis of wedge resection versus stereotactic body radiation therapy for stage IA non-small cell lung cancer.J Thorac Cardiovasc Surg. 2017 Aug;154(2):675-686.e4. doi: 10.1016/j.jtcvs.2017.02.065. Epub 2017 Apr 4. J Thorac Cardiovasc Surg. 2017. PMID: 28461054
-
Lobectomy versus stereotactic body radiotherapy in healthy patients with stage I lung cancer.J Thorac Cardiovasc Surg. 2016 Jul;152(1):44-54.e9. doi: 10.1016/j.jtcvs.2016.03.060. Epub 2016 Apr 7. J Thorac Cardiovasc Surg. 2016. PMID: 27131846
-
Surgery versus stereotactic body radiation therapy for stage I non-small cell lung cancer: A comprehensive review.Cancer. 2018 Feb 15;124(4):667-678. doi: 10.1002/cncr.31196. Epub 2017 Dec 19. Cancer. 2018. PMID: 29266226 Review.
-
Stereotactic ablative radiotherapy versus lobectomy for stage I non-small cell lung cancer: A systematic review.Thorac Cancer. 2018 Mar;9(3):337-347. doi: 10.1111/1759-7714.12574. Epub 2018 Jan 11. Thorac Cancer. 2018. PMID: 29322682 Free PMC article.
Cited by
-
GOECP/SEOR radiotheraphy guidelines for non-small-cell lung cancer.World J Clin Oncol. 2022 Apr 24;13(4):237-266. doi: 10.5306/wjco.v13.i4.237. World J Clin Oncol. 2022. PMID: 35582651 Free PMC article. Review.
-
EXACT-Net: Framework for EHR-Guided Lung Tumor Auto-Segmentation for Non-Small Cell Lung Cancer Radiotherapy.Cancers (Basel). 2024 Dec 6;16(23):4097. doi: 10.3390/cancers16234097. Cancers (Basel). 2024. PMID: 39682283 Free PMC article.
-
Interactions between COVID-19 and Lung Cancer: Lessons Learned during the Pandemic.Cancers (Basel). 2022 Jul 23;14(15):3598. doi: 10.3390/cancers14153598. Cancers (Basel). 2022. PMID: 35892857 Free PMC article. Review.
-
Expression and prongostic impact of galectin-7 in human lung cancer.Medicine (Baltimore). 2024 Oct 4;103(40):e39911. doi: 10.1097/MD.0000000000039911. Medicine (Baltimore). 2024. PMID: 39465762 Free PMC article.
-
Patient-clinician communication and patient-centered outcomes among patients with suspected stage I non-small cell lung cancer: a prospective cohort study.Med Oncol. 2022 Sep 29;39(12):203. doi: 10.1007/s12032-022-01776-y. Med Oncol. 2022. PMID: 36175802
References
-
- Baumann P, Nyman J, Hoyer M, Wennberg B, Gagliardi G, Lax I, et al. Outcome in a prospective phase II trial of medically inoperable stage I non-small-cell lung cancer patients treated with stereotactic body radiotherapy. J Clin Oncol 2009;27:3290–6. - PubMed
-
- Jeppesen SS, Schytte T, Jensen HR, Brink C, Hansen O. Stereotactic body radiation therapy versus conventional radiation therapy in patients with early stage non-small cell lung cancer: an updated retrospective study on local failure and survival rates. Acta Oncol 2013;52:1552–8. - PubMed
-
- Palma D, Visser O, Lagerwaard FJ, Belderbos J, Slotman BJ, Senan S. Impact of introducing stereotactic lung radiotherapy for elderly patients with stage I non-small-cell lung cancer: a population-based time-trend analysis. J Clin Oncol 2010;28:5153–9. - PubMed
-
- Woody NM, Stephans KL, Marwaha G, Djemil T, Videtic GM. Stereotactic Body Radiation Therapy for Non-Small Cell Lung Cancer Tumors Greater Than 5 cm: Safety and Efficacy. Int J Radiat Oncol Biol Phys 2015;92:325–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
