

Predictive Modeling of 30-Day Emergency Hospital Transport of Patients Using a Personal Emergency Response System: Prognostic Retrospective Study
- PMID: 30482741
- PMCID: PMC6290270
- DOI: 10.2196/medinform.9907
Predictive Modeling of 30-Day Emergency Hospital Transport of Patients Using a Personal Emergency Response System: Prognostic Retrospective Study
Abstract
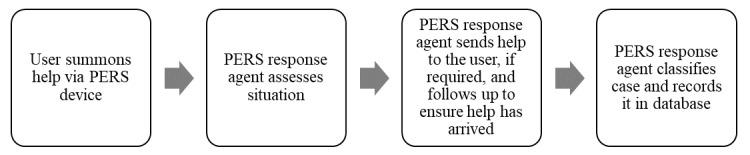
Background: Telehealth programs have been successful in reducing 30-day readmissions and emergency department visits. However, such programs often focus on the costliest patients with multiple morbidities and last for only 30 to 60 days postdischarge. Inexpensive monitoring of elderly patients via a personal emergency response system (PERS) to identify those at high risk for emergency hospital transport could be used to target interventions and prevent avoidable use of costly readmissions and emergency department visits after 30 to 60 days of telehealth use.
Objective: The objectives of this study were to (1) develop and validate a predictive model of 30-day emergency hospital transport based on PERS data; and (2) compare the model's predictions with clinical outcomes derived from the electronic health record (EHR).
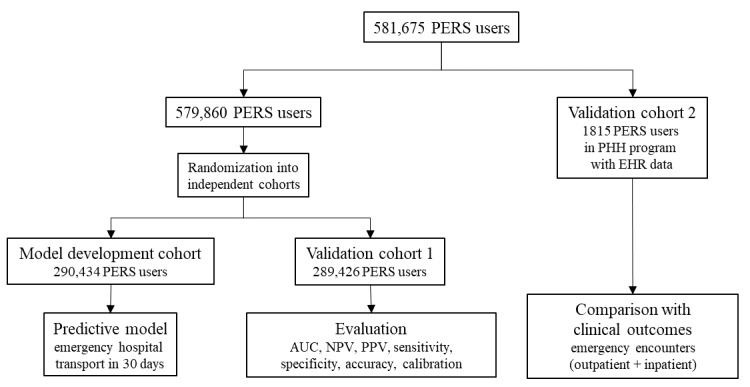
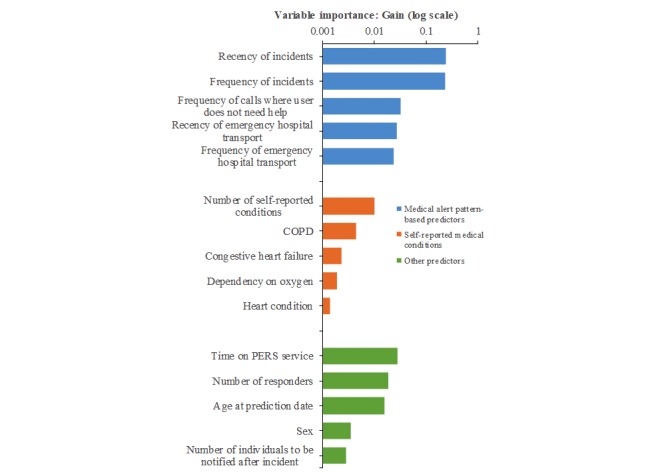
Methods: We used deidentified medical alert pattern data from 290,434 subscribers to a PERS service to build a gradient tree boosting-based predictive model of 30-day hospital transport, which included predictors derived from subscriber demographics, self-reported medical conditions, caregiver network information, and up to 2 years of retrospective PERS medical alert data. We evaluated the model's performance on an independent validation cohort (n=289,426). We linked EHR and PERS records for 1815 patients from a home health care program to compare PERS-based risk scores with rates of emergency encounters as recorded in the EHR.
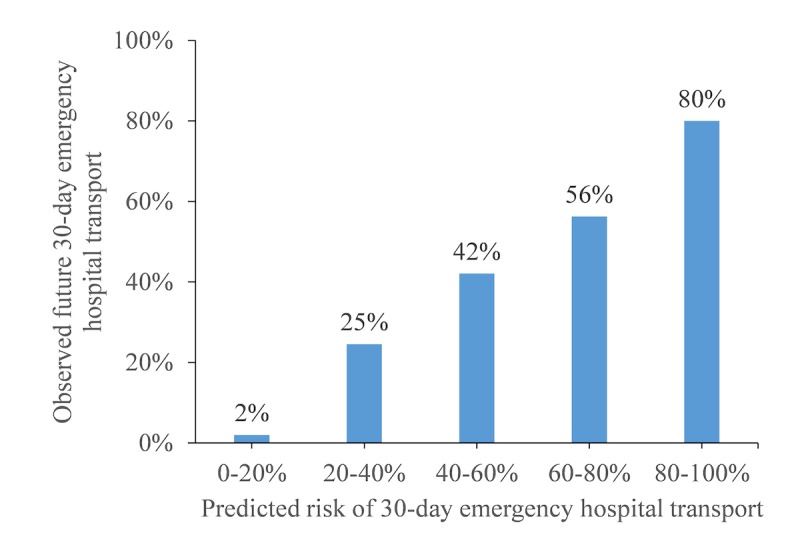
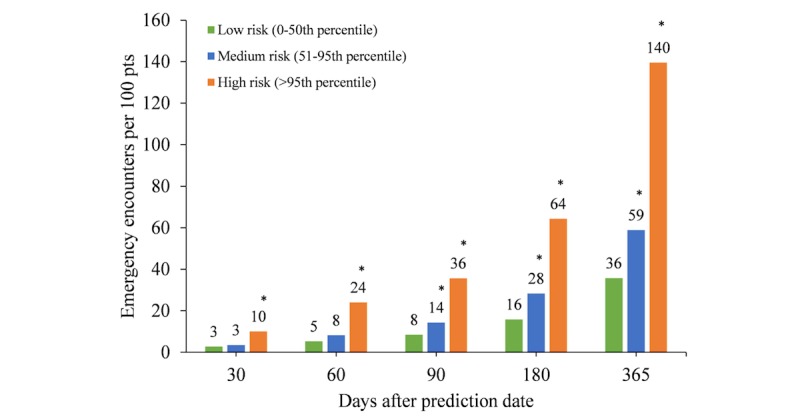
Results: In the validation cohort, 2.22% (6411/289,426) of patients had 1 or more emergency transports in 30 days. The performance of the predictive model of emergency hospital transport, as evaluated by the area under the receiver operating characteristic curve, was 0.779 (95% CI 0.774-0.785). Among the top 1% of predicted high-risk patients, 25.5% had 1 or more emergency hospital transports in the next 30 days. Comparison with clinical outcomes from the EHR showed 3.9 times more emergency encounters among predicted high-risk patients than low-risk patients in the year following the prediction date.
Conclusions: Patient data collected remotely via PERS can be used to reliably predict 30-day emergency hospital transport. Clinical observations from the EHR showed that predicted high-risk patients had nearly four times higher rates of emergency encounters than did low-risk patients. Health care providers could benefit from our validated predictive model by targeting timely preventive interventions to high-risk patients. This could lead to overall improved patient experience, higher quality of care, and more efficient resource utilization.
Keywords: accountable care organizations; decision support techniques; emergency medical dispatch; machine learning; population health.
©Jorn op den Buijs, Mariana Simons, Sara Golas, Nils Fischer, Jennifer Felsted, Linda Schertzer, Stephen Agboola, Joseph Kvedar, Kamal Jethwani. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 27.11.2018.
Conflict of interest statement
Conflicts of Interest: Philips funded the study. JodB, MS, and LS are employed by Philips.
Figures
References
-
- Albert M, McCaig LF, Ashman JJ. Emergency department visits by persons aged 65 and over: United States, 2009-2010. NCHS Data Brief. 2013 Oct;(130):1–8. https://www.cdc.gov/nchs/data/databriefs/db130.pdf - PubMed
-
- Iwata M, Kuzuya M, Kitagawa Y, Iguchi A. Emergency department use by nonagenarian patients. Geriatr Gerontol Int. 2006 Mar;6(1):25–31. doi: 10.1111/j.1447-0594.2006.00310.x. - DOI
LinkOut - more resources
Full Text Sources
