

American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia
- PMID: 30482768
- PMCID: PMC6258919
- DOI: 10.1182/bloodadvances.2018024489
American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia
Abstract
Background: Heparin-induced thrombocytopenia (HIT) is an adverse drug reaction mediated by platelet-activating antibodies that target complexes of platelet factor 4 and heparin. Patients are at markedly increased risk of thromboembolism.
Objective: These evidence-based guidelines of the American Society of Hematology (ASH) are intended to support patients, clinicians, and other health care professionals in their decisions about diagnosis and management of HIT.
Methods: ASH formed a multidisciplinary guideline panel balanced to minimize potential bias from conflicts of interest. The McMaster University GRADE Centre supported the guideline development process, including updating or performing systematic evidence reviews. The panel prioritized clinical questions and outcomes according to their importance for clinicians and patients. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess evidence and make recommendations, which were subject to public comment.
Results: The panel agreed on 33 recommendations. The recommendations address screening of asymptomatic patients for HIT, diagnosis and initial management of patients with suspected HIT, treatment of acute HIT, and special situations in patients with acute HIT or a history of HIT, including cardiovascular surgery, percutaneous cardiovascular intervention, renal replacement therapy, and venous thromboembolism prophylaxis.
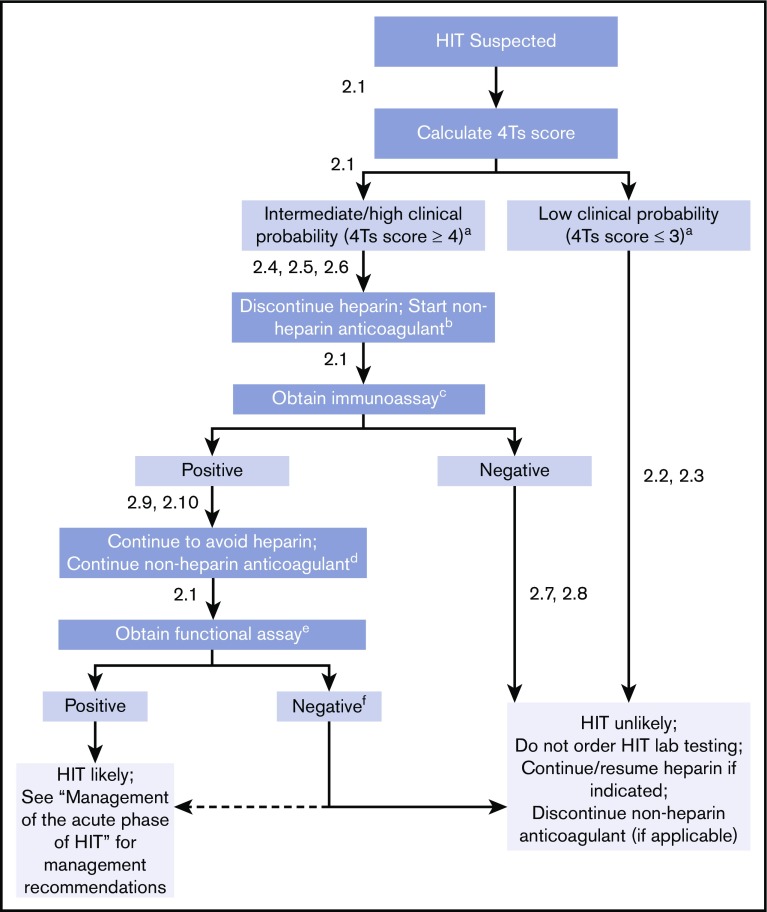
Conclusions: Strong recommendations include use of the 4Ts score rather than a gestalt approach for estimating the pretest probability of HIT and avoidance of HIT laboratory testing and empiric treatment of HIT in patients with a low-probability 4Ts score. Conditional recommendations include the choice among non-heparin anticoagulants (argatroban, bivalirudin, danaparoid, fondaparinux, direct oral anticoagulants) for treatment of acute HIT.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: All authors were members of the guideline panel or members of the systematic review team or both. They completed disclosure-of-interest forms, which were reviewed by ASH and are available as supplements 2 and 3.
Figures
References
-
- Institute of Medicine. Clinical Practice Guidelines We Can Trust. Washington, DC: The National Academies Press; 2011. 10.17226/13058. - DOI
-
- Qaseem A, Forland F, Macbeth F, Ollenschläger G, Phillips S, van der Wees P; Board of Trustees of the Guidelines International Network. Guidelines International Network: toward international standards for clinical practice guidelines. Ann Intern Med. 2012;156(7):525-531. - PubMed
-
- Schünemann HJ, Al-Ansary LA, Forland F, et al. ; Board of Trustees of the Guidelines International Network. Guidelines International Network: principles for disclosure of interests and management of conflicts in guidelines. Ann Intern Med. 2015;163(7):548-553. - PubMed
-
- Alonso-Coello P, Oxman AD, Moberg J, et al. ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016;353:i2089. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
