

Diagnosis and Management of Immune Checkpoint Inhibitor-Associated Neurologic Toxicity: Illustrative Case and Review of the Literature
- PMID: 30482825
- PMCID: PMC6459240
- DOI: 10.1634/theoncologist.2018-0359
Diagnosis and Management of Immune Checkpoint Inhibitor-Associated Neurologic Toxicity: Illustrative Case and Review of the Literature
Abstract
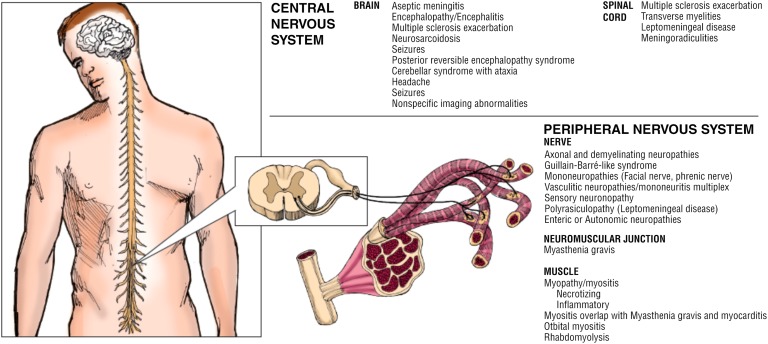
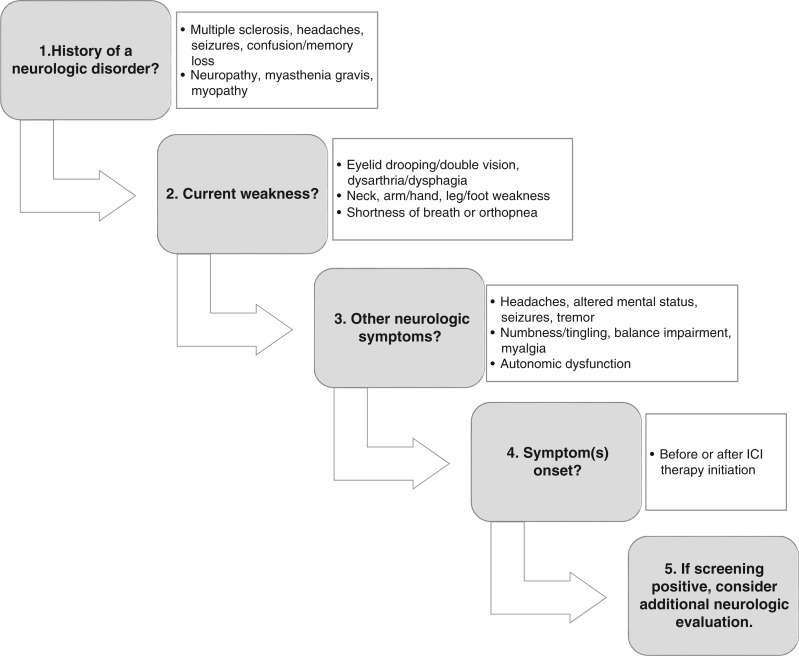
Immune checkpoint inhibitors (ICIs) initiate antitumor immunity by blocking the action of immune inhibitor-signaled cytotoxic proteins, such as cytotoxic T-lymphocyte-associated protein 4, programmed cell death protein 1, and programmed cell death ligand 1. However, in rare cases (∼1%-12% of patients), ICI treatment causes neurologic immune-related adverse events (irAEs). These include, but are not limited to, headache, encephalitis, neuropathies, myasthenia gravis, and myositis. The symptoms associated with irAEs can range from mild (grade 1-2) to severe (grade 3-4); however, they are often challenging to diagnose because they may present as generalized symptoms, such as fatigue and weakness, that can also be caused by the cancer itself. Here, we present an illustrative case of a 67-year-old woman who presented with signs of a neurologic irAE, including progressive dysphagia and weakness leading to falls, which started during treatment with pembrolizumab and worsened following initiation of ipilimumab. Following neurological and pathological evaluation, she was diagnosed with myositis. She was treated with steroids and improved rapidly. In this article, we review previous literature to provide guidance to frequently asked questions concerning the diagnosis and management of neurologic irAEs in patients with advanced cancer. With prompt and effective treatment, most patients will achieve a complete recovery. KEY POINTS: Neurologic immune-related adverse events (irAEs) affect approximately 1% of patients treated with immune checkpoint inhibitor (ICI) monotherapy and 2%-3% treated with combination therapy. These irAEs can affect any portion of the nervous system, although peripheral nerve system manifestations are most common. Overlap syndromes with multiple neurologic irAEs or other affected organ systems frequently exist.Diagnosis of neurologic irAEs can be challenging. Routine testing may be unremarkable and symptoms frequently mimic those from cancer or side effects of other therapies. Optimal management is currently unknown. A systematic, highly coordinated, and multidisciplinary approach is critical.Outcomes from neurologic irAEs are typically favorable with the current practice of holding the ICI and starting corticosteroids. Some patients are even successfully retreated with an ICI. A subset of patients, however, have a fulminant and potentially fatal course.Improved risk assessments and targeted therapies are needed.
© AlphaMed Press 2018.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Daud A, Robert C, Hodi FS et al. Long‐term efficacy of pembrolizumab (pembro; MK‐3475) in a pooled analysis of 655 patients (pts) with advanced melanoma (MEL) enrolled in KEYNOTE‐001. J Clin Oncol 2015;33(suppl 15);9005a.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
