

Global epidemiology and holistic prevention of pancreatitis
- PMID: 30482911
- PMCID: PMC6597260
- DOI: 10.1038/s41575-018-0087-5
Global epidemiology and holistic prevention of pancreatitis
Abstract
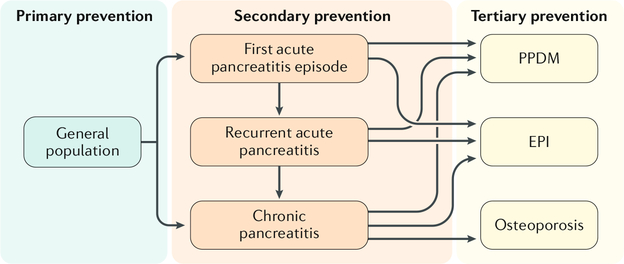
Knowledge of pancreatitis in the 20th century was shaped predominantly by animal data and clinical trials. Several large general population-based cohort studies and comprehensive systematic literature reviews in the 21st century have had a major effect on our understanding of pancreatitis and its sequelae. This Review provides precise and up-to-date data on the burden of acute pancreatitis, chronic pancreatitis and post-pancreatitis diabetes mellitus. Exocrine pancreatic insufficiency and altered bone metabolism following pancreatitis are also discussed. Furthermore, the article introduces a framework for the holistic prevention of pancreatitis with a view to providing guidance on strategies and intervention objectives at primary, secondary and tertiary levels. Concerted efforts by not only gastroenterologists and surgeons but also primary care physicians, endocrinologists, radiologists, pain specialists, dietitians, epidemiologists and public health specialists will be required to reduce meaningfully the burden of pancreatitis and its sequelae over the ensuing decades.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
References
-
- Petrov MS Abdominal fat: a key player in metabolic acute pancreatitis. Am. J. Gastroenterol 108, 140–142 (2013). - PubMed
-
- Yadav D, Papachristou GI & Whitcomb DC Alcohol-associated pancreatitis. Gastroenterol. Clin. North Am 36, 219–238 (2007). - PubMed
-
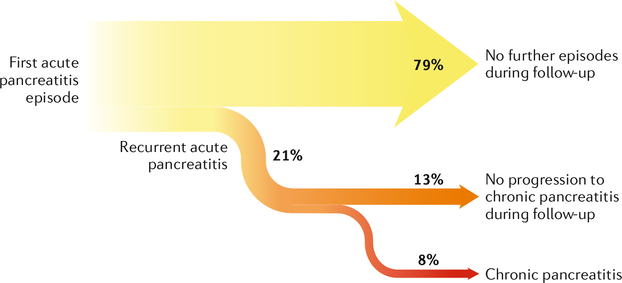
- Sankaran SJ et al. Frequency of progression from acute to chronic pancreatitis and risk factors: a meta-analysis. Gastroenterology 149, 1490–1500 (2015). - PubMed
-
- DeSouza SV et al. Pancreas volume in health and disease: a systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol 12, 757–766 (2018). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
