

Evolution of Cancer Pharmacological Treatments at the Turn of the Third Millennium
- PMID: 30483135
- PMCID: PMC6243123
- DOI: 10.3389/fphar.2018.01300
Evolution of Cancer Pharmacological Treatments at the Turn of the Third Millennium
Abstract
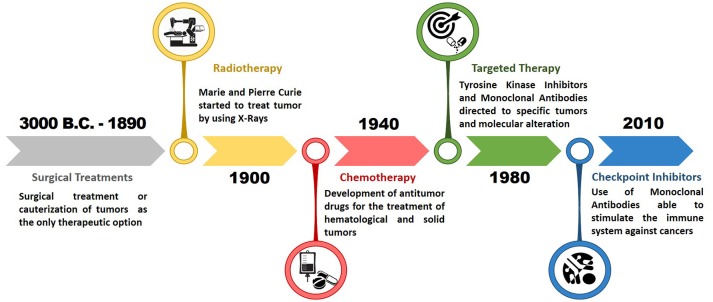
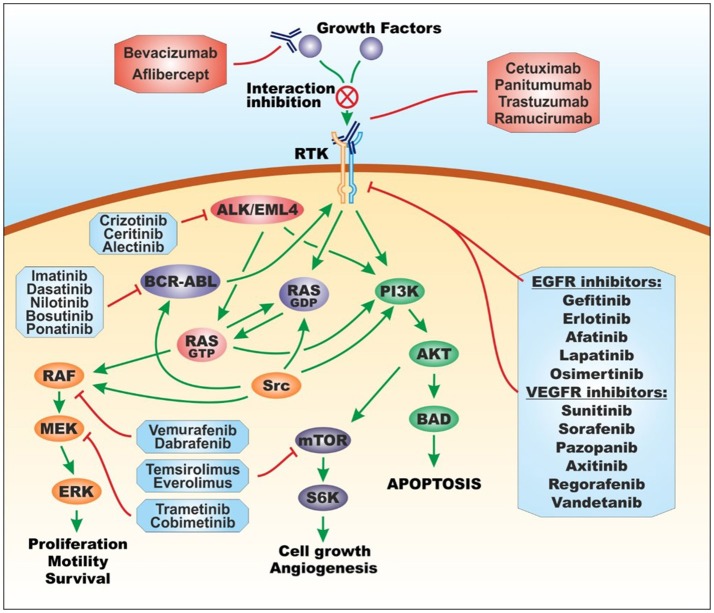
The medical history of cancer began millennia ago. Historical findings of patients with cancer date back to ancient Egyptian and Greek civilizations, where this disease was predominantly treated with radical surgery and cautery that were often ineffective, leading to the death of patients. Over the centuries, important discoveries allowed to identify the biological and pathological features of tumors, without however contributing to the development of effective therapeutic approaches until the end of the 1800s, when the discovery of X-rays and their use for the treatment of tumors provided the first modern therapeutic approach in medical oncology. However, a real breakthrough took place after the Second World War, with the discovery of cytotoxic antitumor drugs and the birth of chemotherapy for the treatment of various hematological and solid tumors. Starting from this epochal turning point, there has been an exponential growth of studies concerning the use of new drugs for cancer treatment. The second fundamental breakthrough in the field of oncology and pharmacology took place at the beginning of the '80s, thanks to molecular and cellular biology studies that allowed the development of specific drugs for some molecular targets involved in neoplastic processes, giving rise to targeted therapy. Both chemotherapy and target therapy have significantly improved the survival and quality of life of cancer patients inducing sometimes complete tumor remission. Subsequently, at the turn of the third millennium, thanks to genetic engineering studies, there was a further advancement of clinical oncology and pharmacology with the introduction of monoclonal antibodies and immune checkpoint inhibitors for the treatment of advanced or metastatic tumors, for which no effective treatment was available before. Today, cancer research is always aimed at the study and development of new therapeutic approaches for cancer treatment. Currently, several researchers are focused on the development of cell therapies, anti-tumor vaccines, and new biotechnological drugs that have already shown promising results in preclinical studies, therefore, in the near future, we will certainly assist to a new revolution in the field of medical oncology.
Keywords: antineoplastic drugs; cancer; cell therapy; chemotherapy; targeted therapy.
Figures
References
-
- Abdel-Monem M. M., Newton N. E., Weeks C. E. (1974). Inhibitors of polyamine biosynthesis. 1. Alpha-methyl-(plus or minus)-ornithine, an inhibitor of ornithine decarboxylase. J. Med. Chem. 17, 447–451. - PubMed
-
- Aboud-Pirak E., Hurwitz E., Pirak M. E., Bellot F., Schlessinger J., Sela M. (1988). Efficacy of antibodies to epidermal growth factor receptor against KB carcinoma in vitro and in nude mice. J. Natl. Cancer Inst. 80, 1605–1611. - PubMed
-
- ACTIP (2017). Animal Cell Technology Industrial Platform. Monoclonal Antibodies Approved by the EMA and FDA for Therapeutic Use status (2017). Available online at: http://www.actip.org/products/monoclonal-antibodies-approved-by-the-ema-...
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources