

High Therapeutic Efficacy of a New Survivin LSP-Cancer Vaccine Containing CD4+ and CD8+ T-Cell Epitopes
- PMID: 30483475
- PMCID: PMC6243131
- DOI: 10.3389/fonc.2018.00517
High Therapeutic Efficacy of a New Survivin LSP-Cancer Vaccine Containing CD4+ and CD8+ T-Cell Epitopes
Abstract
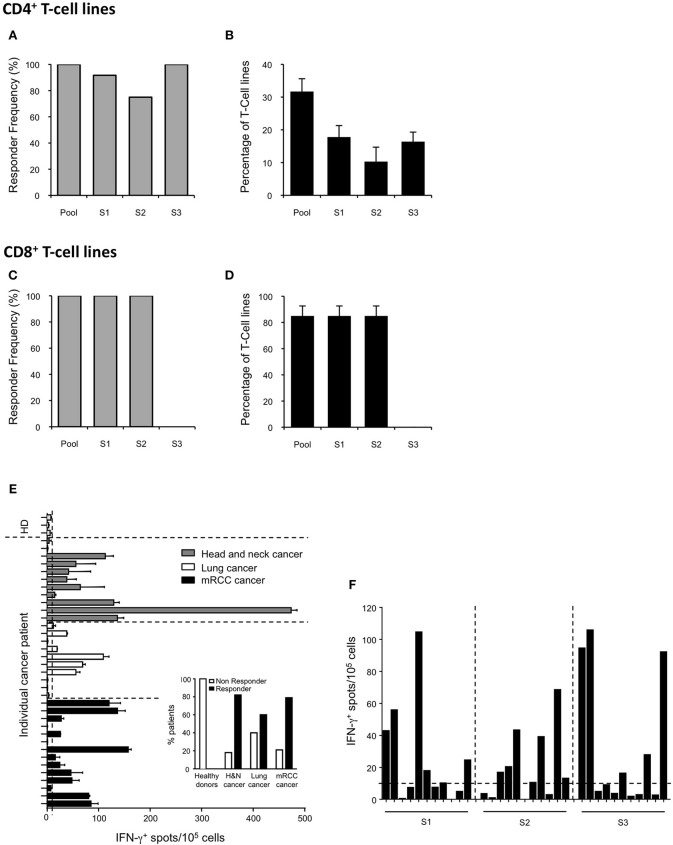
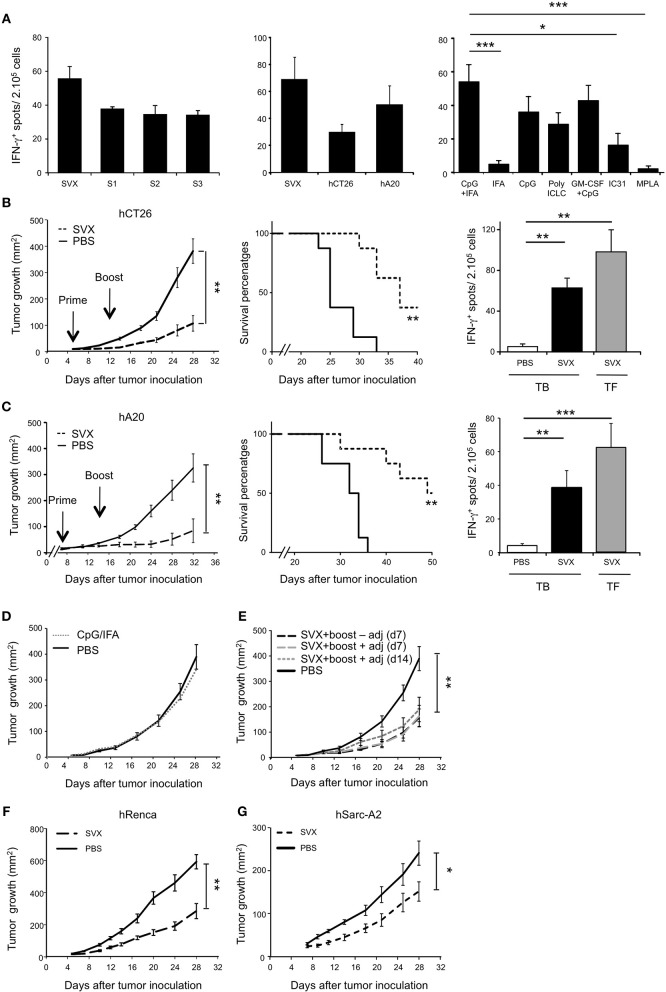
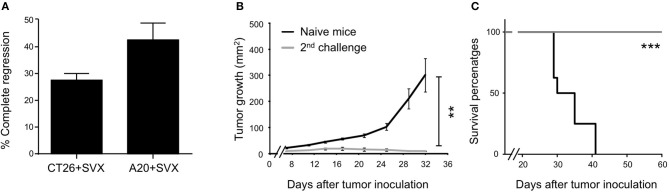
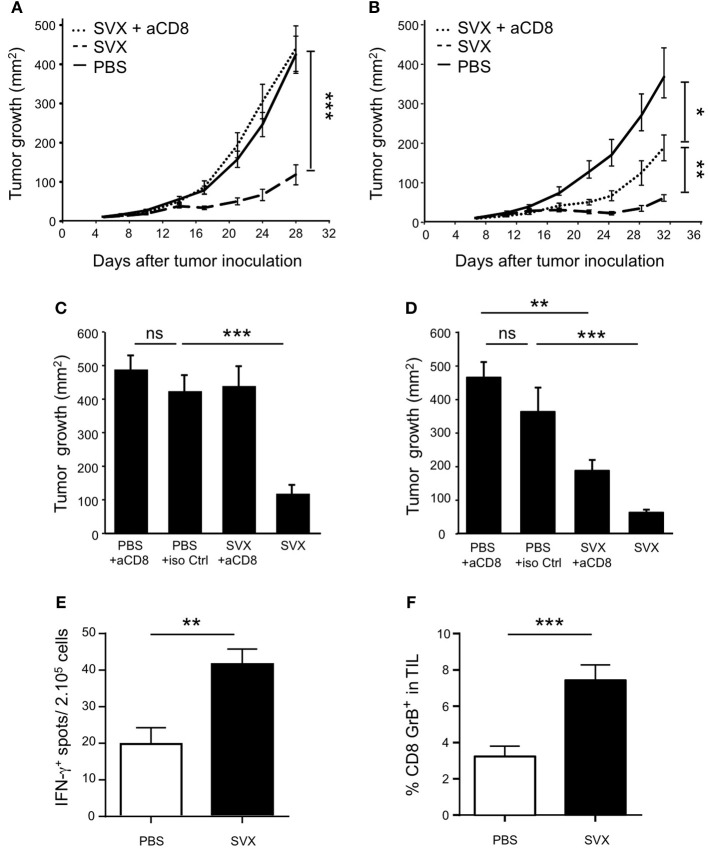
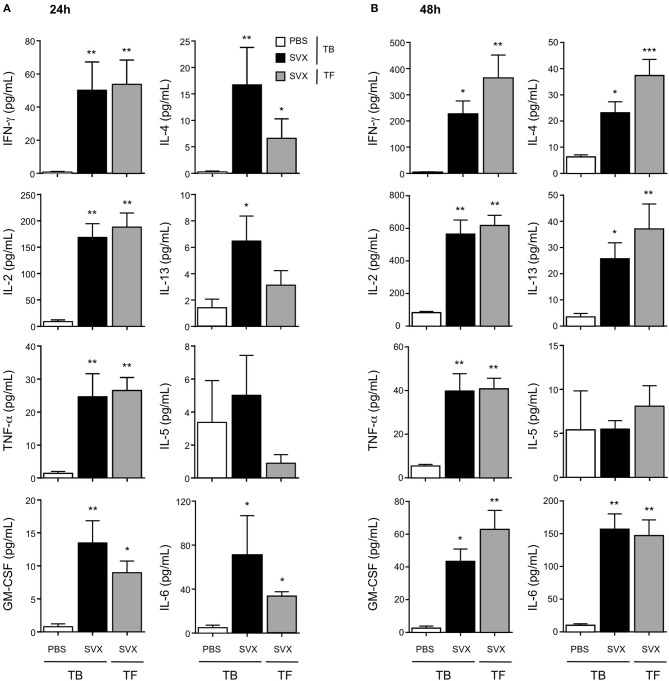
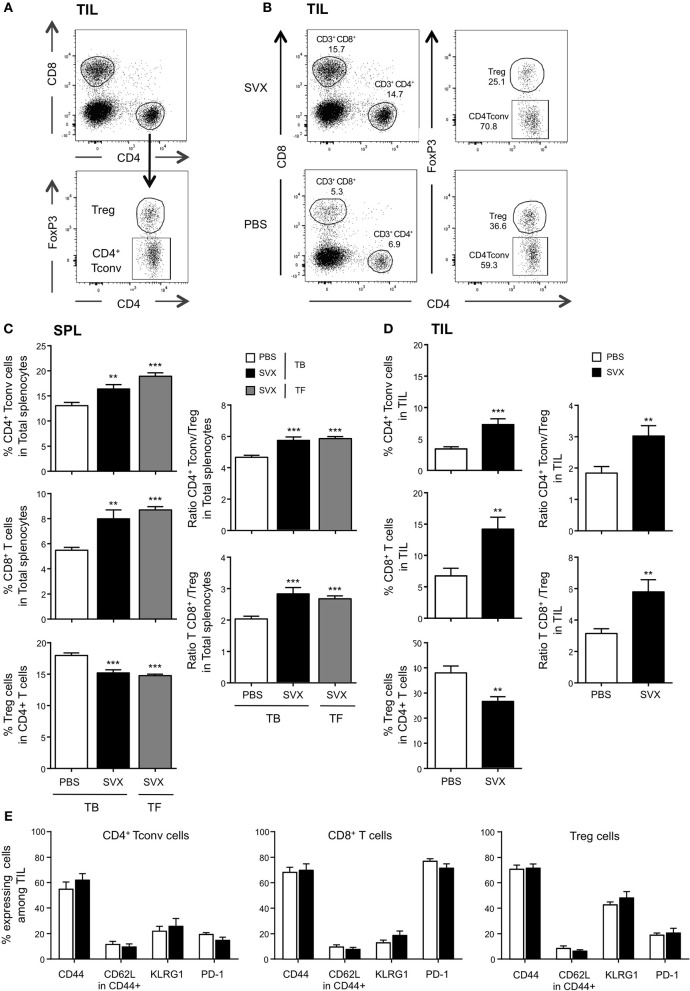
The efficacy of an antitumoral vaccine relies both on the choice of the antigen targeted and on its design. The tumor antigen survivin is an attractive target to develop therapeutic cancer vaccines because of its restricted over-expression and vital functions in most human tumors. Accordingly, several clinical trials targeting survivin in various cancer indications have been conducted. Most of them relied on short peptide-based vaccines and showed promising, but limited clinical results. In this study, we investigated the immunogenicity and therapeutic efficacy of a new long synthetic peptide (LSP)-based cancer vaccine targeting the tumor antigen survivin (SVX). This SVX vaccine is composed of three long synthetic peptides containing several CD4+ and CD8+ T-cell epitopes, which bind to various HLA class II and class I molecules. Studies in healthy individuals showed CD4+ and CD8+ T-cell immunogenicity of SVX peptides in human, irrespective of the individual's HLA types. Importantly, high frequencies of spontaneous T-cell precursors specific to SVX peptides were also detected in the blood of various cancer patients, demonstrating the absence of tolerance against these peptides. We then demonstrated SVX vaccine's high therapeutic efficacy against four different established murine tumor models, associated with its capacity to generate both specific cytotoxic CD8+ and multifunctional Th1 CD4+ T-cell responses. When tumors were eradicated, generated memory T-cell responses protected against rechallenge allowing long-term protection against relapses. Treatment with SVX vaccine was also found to reshape the tumor microenvironment by increasing the tumor infiltration of both CD4+ and CD8+ T cells but not Treg cells therefore tipping the balance toward a highly efficient immune response. These results highlight that this LSP-based SVX vaccine appears as a promising cancer vaccine and warrants its further clinical development.
Keywords: T-cell responses; cancer vaccine; immunotherapy; long synthetic peptide; tumor associated survivin antigen.
Figures
Similar articles
-
Identification of novel helper epitope peptides of Survivin cancer-associated antigen applicable to developing helper/killer-hybrid epitope long peptide cancer vaccine.Immunol Lett. 2014 Sep;161(1):20-30. doi: 10.1016/j.imlet.2014.04.010. Epub 2014 Apr 30. Immunol Lett. 2014. PMID: 24794408 Clinical Trial.
-
Identification of a promiscuous HLA DR-restricted T-cell epitope derived from the inhibitor of apoptosis protein survivin.Hum Immunol. 2007 Jul;68(7):572-6. doi: 10.1016/j.humimm.2007.03.007. Epub 2007 Apr 11. Hum Immunol. 2007. PMID: 17584578
-
Peptide epitopes from the Wilms' tumor 1 oncoprotein stimulate CD4+ and CD8+ T cells that recognize and kill human malignant mesothelioma tumor cells.Clin Cancer Res. 2007 Aug 1;13(15 Pt 1):4547-55. doi: 10.1158/1078-0432.CCR-07-0708. Clin Cancer Res. 2007. PMID: 17671141
-
Immune modulations during chemoimmunotherapy & novel vaccine strategies--in metastatic melanoma and non small-cell lung cancer.Dan Med J. 2013 Dec;60(12):B4774. Dan Med J. 2013. PMID: 24355457 Review.
-
Survivin-derived peptide epitopes and their role for induction of antitumor immunity in hematological malignancies.Leuk Lymphoma. 2006 Jun;47(6):978-85. doi: 10.1080/10428190500464062. Leuk Lymphoma. 2006. PMID: 16840186 Review.
Cited by
-
Generation of multiepitope cancer vaccines based on large combinatorial libraries of survivin-derived mutant epitopes.Immunology. 2020 Oct;161(2):123-138. doi: 10.1111/imm.13233. Epub 2020 Aug 3. Immunology. 2020. PMID: 32619293 Free PMC article.
-
Recent Advances in Cancer Vaccines: Challenges, Achievements, and Futuristic Prospects.Vaccines (Basel). 2022 Nov 25;10(12):2011. doi: 10.3390/vaccines10122011. Vaccines (Basel). 2022. PMID: 36560420 Free PMC article. Review.
-
Autoantibodies in cancer: a systematic review of their clinical role in the most prevalent cancers.Front Immunol. 2024 Aug 21;15:1455602. doi: 10.3389/fimmu.2024.1455602. eCollection 2024. Front Immunol. 2024. PMID: 39234247 Free PMC article.
-
Cancer Vaccines: Promising Therapeutics or an Unattainable Dream.Vaccines (Basel). 2021 Jun 18;9(6):668. doi: 10.3390/vaccines9060668. Vaccines (Basel). 2021. PMID: 34207062 Free PMC article. Review.
-
Potential Mechanisms for Immunotherapy Resistance in Adult Soft-Tissue Sarcoma.Target Oncol. 2025 May;20(3):485-502. doi: 10.1007/s11523-025-01145-5. Epub 2025 Apr 27. Target Oncol. 2025. PMID: 40289241 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials