

Treatment of fecal impaction in children using combined polyethylene glycol and sodium picosulphate
- PMID: 30483580
- PMCID: PMC6207039
- DOI: 10.1002/jgh3.12062
Treatment of fecal impaction in children using combined polyethylene glycol and sodium picosulphate
Abstract
Background and aim: Polyethylene glycol (PEG) is the gold standard for fecal disimpaction in constipation. A regimen of PEG combined with the stimulant laxative sodium picosulphate (SPS) produced fecal disimpaction in chronically constipated children in the community, but it is unknown if it is effective for more severe constipation. To determine the stool output and effect of a combined PEG and SPS regimen on fecaloma in children with severe constipation and impaction.
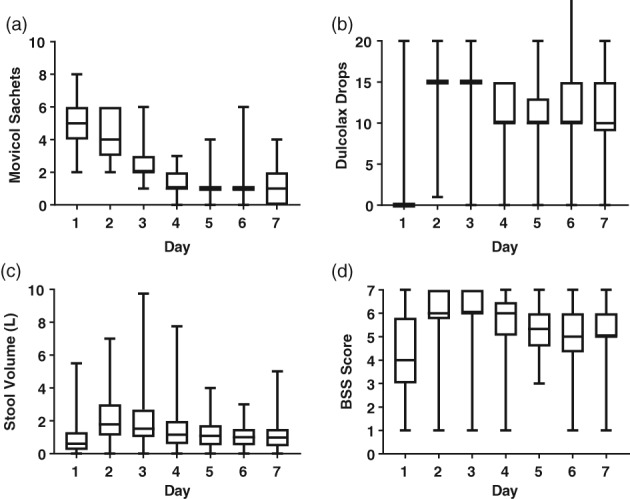
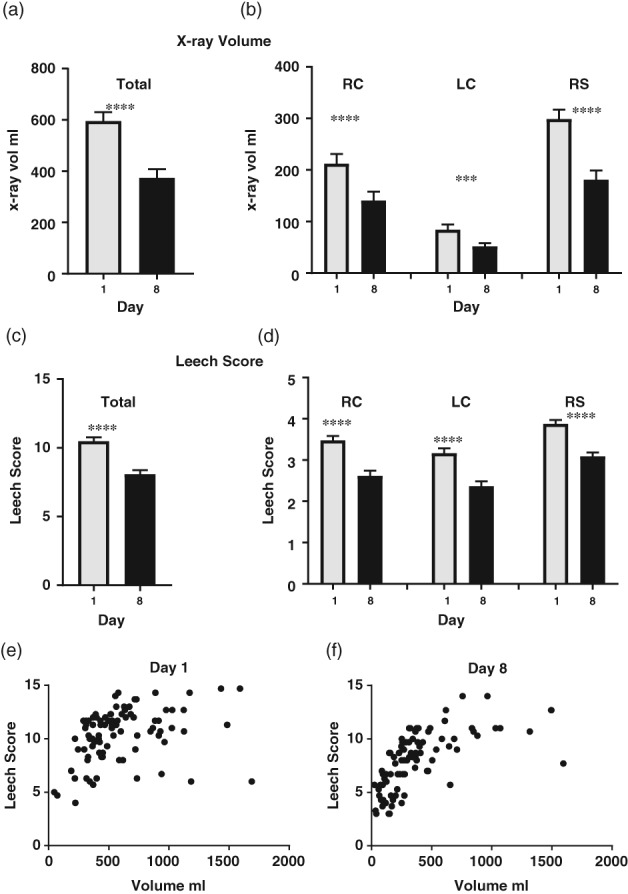
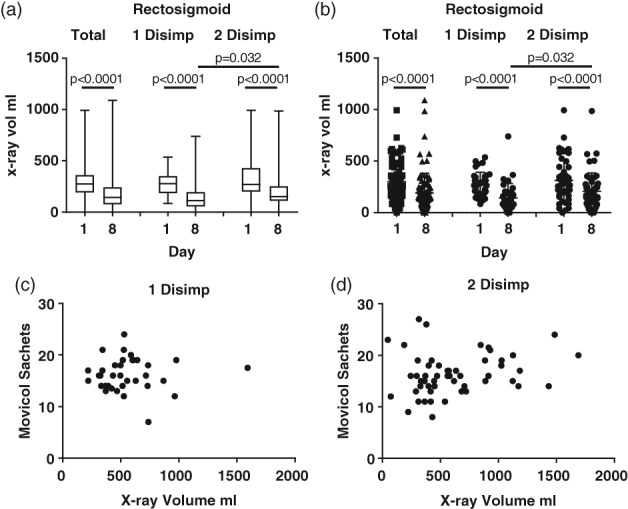
Methods: Children with symptoms for a duration of ≥2 years, a palpable fecaloma, and enlarged rectum on X-ray (rectal: pelvic ratio > 0.6) were recruited from a tertiary hospital. Daily diaries recorded laxative dose, stool frequency, volume, and consistency (Bristol stool scale, BSS). Abdominal X-rays were taken on day 1 and day 8, and stool loading was assessed using the Leech score. Laxative doses were based on the child's age. The dose of PEG with electrolytes taken was 2-8 sachets (14.7 g/sachet) on days 1-2, reducing to 2-6 sachets on day 3. The SPS dose was 15-20 drops on days 2-3.
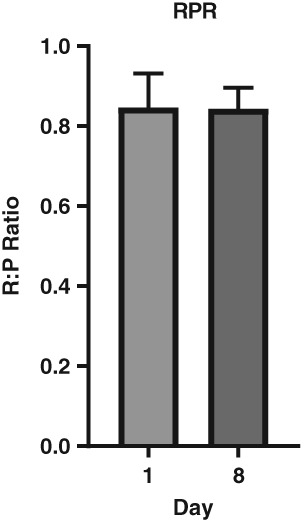
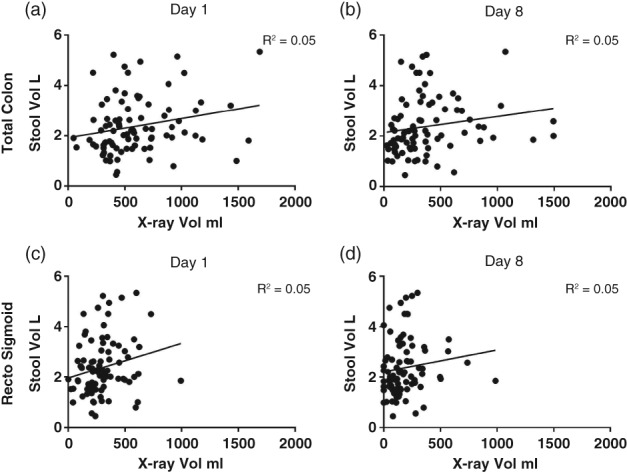
Results: Eighty-nine children (4-18 years) produced a large volume of soft stool (median/inter-quartile-range: 2.2/1.6-3.1 L) over 7 days. Stool volume on X-rays decreased significantly in the colon (P < 0.001). Fecalomas resolved in 40 of 89 children, while 49 needed a second high dose. Rectal:pelvic ratios did not change.
Conclusions: A combined high dose of PEG and SPS on days 1 and 2 was effective in removing the fecaloma in half of the children. Administering high doses for a longer period should be tested to provide outpatient disimpaction for severe fecalomas. Rectums remained flaccid after emptying.
Keywords: X‐rays; chronic constipation; laxatives; macrogol; polyethylene glycol.
Figures
Similar articles
-
Disimpaction of children with severe constipation in 3-4 days in a suburban clinic using polyethylene glycol with electrolytes and sodium picosulphate.J Paediatr Child Health. 2015 Dec;51(12):1195-8. doi: 10.1111/jpc.12939. Epub 2015 Jun 8. J Paediatr Child Health. 2015. PMID: 26059611
-
Efficacy and tolerability of peg-only laxative on faecal impaction and chronic constipation in children. A controlled double blind randomized study vs a standard peg-electrolyte laxative.BMC Pediatr. 2012 Nov 15;12:178. doi: 10.1186/1471-2431-12-178. BMC Pediatr. 2012. PMID: 23152962 Free PMC article. Clinical Trial.
-
Evaluation of polyethylene glycol plus electrolytes in the treatment of severe constipation and faecal impaction in adults.Curr Med Res Opin. 2005 Oct;21(10):1595-602. doi: 10.1185/030079905X65385. Curr Med Res Opin. 2005. PMID: 16238899
-
Cochrane Review: Osmotic and stimulant laxatives for the management of childhood constipation (Review).Evid Based Child Health. 2013 Jan;8(1):57-109. doi: 10.1002/ebch.1893. Evid Based Child Health. 2013. PMID: 23878124 Review.
-
Use of polyethylene glycol in functional constipation and fecal impaction.Rev Esp Enferm Dig. 2016 Dec;108(12):790-806. doi: 10.17235/reed.2016.4571/2016. Rev Esp Enferm Dig. 2016. PMID: 27871178 Review.
Cited by
-
The ten "hard" questions in pediatric functional constipation.Ital J Pediatr. 2024 Apr 8;50(1):64. doi: 10.1186/s13052-024-01623-y. Ital J Pediatr. 2024. PMID: 38649896 Free PMC article. Review.
-
Large Bowel Obstruction Secondary to a Fecaloma in a Child With Cerebral Palsy.Cureus. 2022 Nov 4;14(11):e31078. doi: 10.7759/cureus.31078. eCollection 2022 Nov. Cureus. 2022. PMID: 36475161 Free PMC article.
-
An Update of Pharmacological Management in Children with Functional Constipation.Paediatr Drugs. 2023 May;25(3):343-358. doi: 10.1007/s40272-023-00563-0. Epub 2023 Mar 20. Paediatr Drugs. 2023. PMID: 36941393 Free PMC article. Review.
References
-
- van den Berg MM, Benninga MA, Di Lorenzo C. Epidemiology of childhood constipation: a systematic review. Am. J. Gastroenterol. 2006; 101: 2401–9. - PubMed
-
- Mugie SM, Benninga MA, Di Lorenzo C. Epidemiology of constipation in children and adults: a systematic review. Best Pract. Res. Clin. Gastroenterol. 2011; 25: 3–18. - PubMed
-
- Quigley EMM. Definition and epidemiology In: Southwell BR, Hutson JM, eds. Constipation: Current and Emerging Treatments. London: Future Medicine, 2013; 7–15.
-
- Tabbers MM, Dilorenzo C, Berger MY et al Evaluation and treatment of functional constipation in infants and children: evidence‐based recommendations from ESPGHAN and NASPGHAN. J. Pediatr. Gastroenterol. Nutr. 2014; 58: 265–81. - PubMed
-
- Bharucha AE, Dorn SD, Lembo A, Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology. 2013; 144: 211–7. - PubMed
LinkOut - more resources
Full Text Sources
