

Imaging of thoracic hernias: types and complications
- PMID: 30484078
- PMCID: PMC6269341
- DOI: 10.1007/s13244-018-0670-x
Imaging of thoracic hernias: types and complications
Abstract
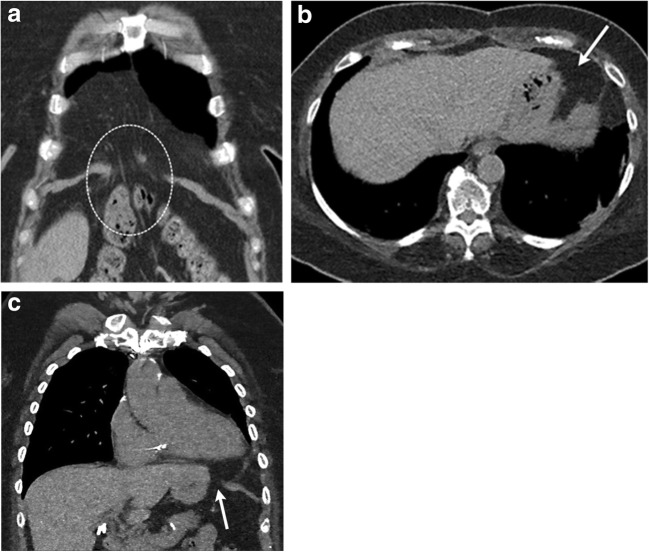
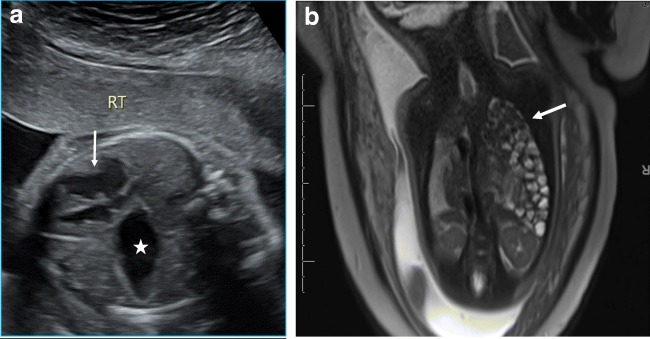
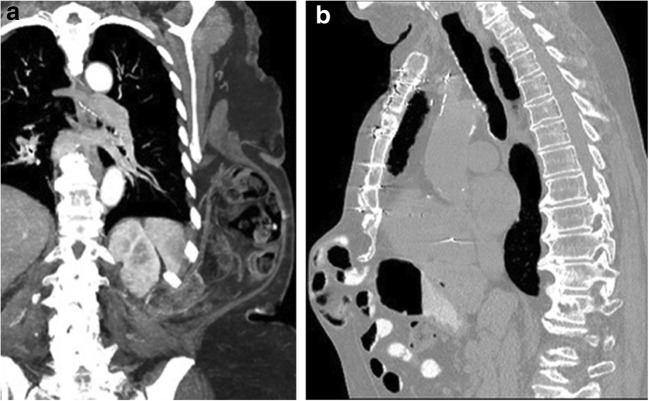
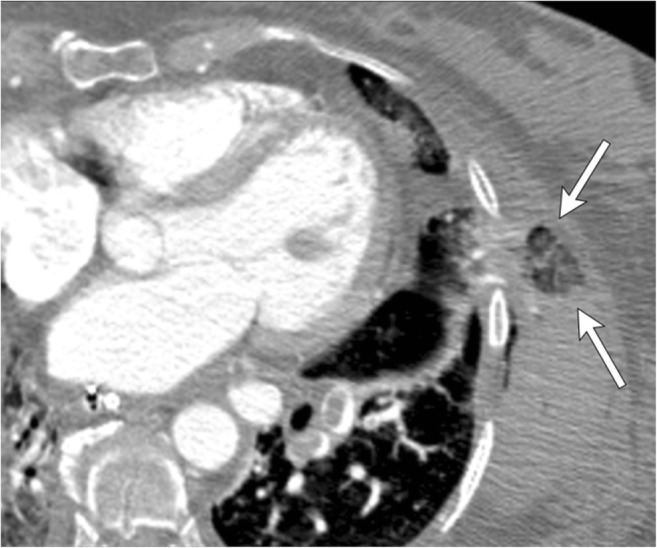
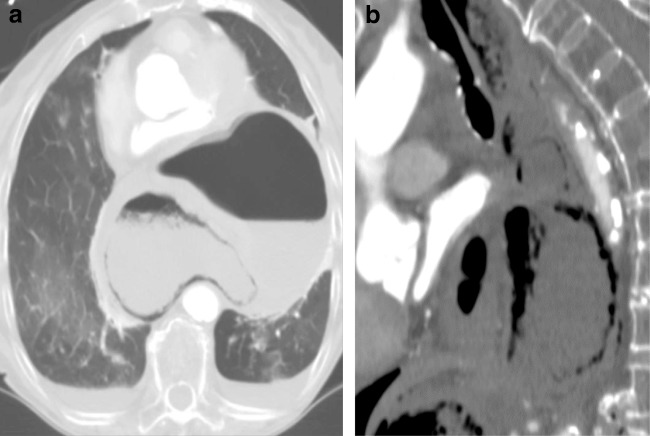
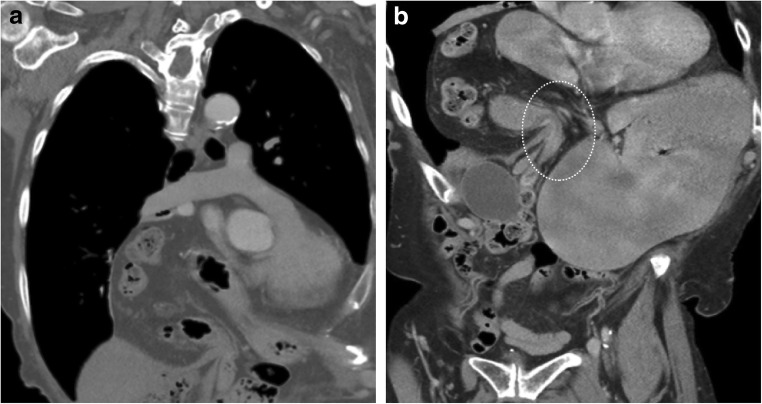
Thoracic hernias are characterised by either protrusion of the thoracic contents outside their normal anatomical confines or extension of the abdominal contents within the thorax. Thoracic hernias can be either congenital or acquired in aetiology. They can occur at the level of the thoracic inlet, chest wall or diaphragm. Thoracic hernias can be symptomatic or fortuitously discovered on imaging obtained for other indications. Complications of thoracic hernias include incarceration, trauma and strangulation with necrosis. Multiple imaging modalities are available to evaluate thoracic hernias. Radiographs usually offer the first clue to the diagnosis. Upper gastrointestinal radiography can identify bowel herniation and associated complications. CT and occasionally MR can be useful for further evaluation of these abnormalities, accurately identifying the type of hernia, its contents, associated complications, and provide a roadmap for surgical planning. In this article, we review the different types of thoracic hernias and the role of imaging in the evaluation of these hernias. TEACHING POINTS: • Protrusion of lung contents beyond the anatomic confines of the thorax constitutes a hernia. • Complications of thoracic hernias include incarceration, trauma and strangulation with necrosis. • Multiple imaging modalities are available to evaluate thoracic hernias. • CT is the imaging modality of choice for identifying thoracic hernias and their complications. • Imaging can provide a roadmap for surgical planning.
Keywords: Diaphragmatic hernia; Lung hernia; Pericardial hernia; Sternal dehiscence.
Figures









Similar articles
-
Imaging of abdominal hernias.Radiographics. 1995 Mar;15(2):333-47. doi: 10.1148/radiographics.15.2.7761639. Radiographics. 1995. PMID: 7761639
-
Diaphragmatic Hernia.2025 Jan 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jan 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30725637 Free Books & Documents.
-
Congenital and acquired lung hernias.J Thorac Imaging. 1996 Winter;11(1):75-82. doi: 10.1097/00005382-199601110-00008. J Thorac Imaging. 1996. PMID: 8770830 Review.
-
Thoracic hernias: What the radiologist should know.J Med Imaging Radiat Oncol. 2025 Feb;69(1):62-71. doi: 10.1111/1754-9485.13792. Epub 2024 Oct 18. J Med Imaging Radiat Oncol. 2025. PMID: 39423346 Review.
-
Intestinal obstruction caused by a strangulated Morgagni hernia in an adult patient.J Thorac Imaging. 2005 Aug;20(3):220-2. doi: 10.1097/01.rti.0000154078.59689.36. J Thorac Imaging. 2005. PMID: 16077338
Cited by
-
Imaging findings of lesions in the middle and posterior mediastinum.Jpn J Radiol. 2021 Jan;39(1):15-31. doi: 10.1007/s11604-020-01025-0. Epub 2021 Jan 18. Jpn J Radiol. 2021. PMID: 32740793 Review.
-
Spontaneous intercostal herniation of lung and pleural fluid.Respir Med Case Rep. 2023 Oct 7;46:101925. doi: 10.1016/j.rmcr.2023.101925. eCollection 2023. Respir Med Case Rep. 2023. PMID: 37869609 Free PMC article.
-
Upfront Thoracic Magnetic Resonance Imaging for the Evaluation of Thymic Lesions to Reduce Non-Therapeutic Diagnostic Thymectomy: A Narrative Review.Healthcare (Basel). 2024 Oct 14;12(20):2036. doi: 10.3390/healthcare12202036. Healthcare (Basel). 2024. PMID: 39451451 Free PMC article. Review.
-
Imaging of abdominopelvic oncologic emergencies.Abdom Radiol (NY). 2024 Mar;49(3):823-841. doi: 10.1007/s00261-023-04112-8. Epub 2023 Nov 28. Abdom Radiol (NY). 2024. PMID: 38017112 Review.
-
Acute Gastric Volvulus in the Setting of a Paraesophageal Hernia With Hemoperitoneum: Emergency Department Diagnosis and Management.Cureus. 2021 Dec 14;13(12):e20404. doi: 10.7759/cureus.20404. eCollection 2021 Dec. Cureus. 2021. PMID: 35047248 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
