

Association of Race/Ethnicity With Oral Anticoagulant Use in Patients With Atrial Fibrillation: Findings From the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II
- PMID: 30484833
- PMCID: PMC6583087
- DOI: 10.1001/jamacardio.2018.3945
Association of Race/Ethnicity With Oral Anticoagulant Use in Patients With Atrial Fibrillation: Findings From the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II
Abstract
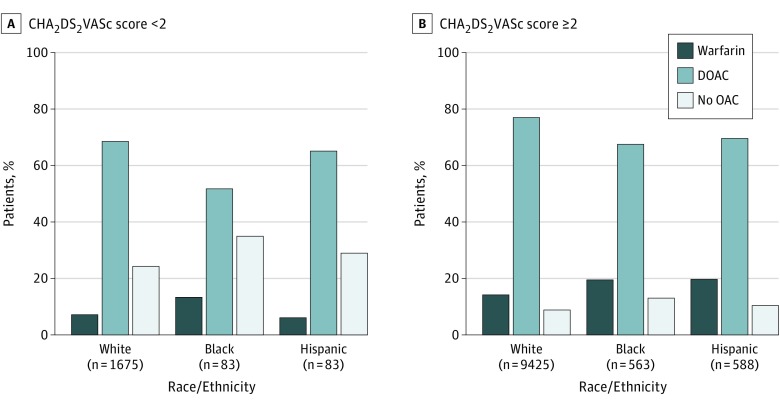
Importance: Black and Hispanic patients are less likely than white patients to use oral anticoagulants for atrial fibrillation. Little is known about racial/ethnic differences in use of direct-acting oral anticoagulants (DOACs) for atrial fibrillation.
Objective: To assess racial/ethnic differences in the use of oral anticoagulants, particularly DOACs, in patients with atrial fibrillation.
Design, setting, and participants: This cohort study used data from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II, a prospective, US-based registry of outpatients with nontransient atrial fibrillation 21 years and older who were followed up from February 2013 to July 2016. Data were analyzed from February 2017 to February 2018.
Exposures: Self-reported race/ethnicity as white, black, or Hispanic.
Main outcomes and measures: The primary outcome was use of any oral anticoagulant, particularly DOACs. Secondary outcomes included the quality of anticoagulation received and oral anticoagulant discontinuation at 1 year.
Results: Of 12 417 patients, 11 100 were white individuals (88.6%), 646 were black individuals (5.2%), and 671 were Hispanic individuals (5.4%) with atrial fibrillation. After adjusting for clinical features, black individuals were less likely to receive any oral anticoagulant than white individuals (adjusted odds ratio [aOR], 0.75 [95% CI, 0.56, 0.99]) and less likely to receive DOACs if an anticoagulant was prescribed (aOR, 0.63 [95% CI, 0.49-0.83]). After further controlling for socioeconomic factors, oral anticoagulant use was no longer significantly different in black individuals (aOR, 0.78 [95% CI, 0.59-1.04]); among patients using oral anticoagulants, DOAC use remained significantly lower in black individuals (aOR, 0.73 [95% CI, 0.55-0.95]). There was no significant difference between white and Hispanic groups in use of oral anticoagulants. Among patients receiving warfarin, the median time in therapeutic range was lower in black individuals (57.1% [IQR, 39.9%-72.5%]) and Hispanic individuals (51.7% [interquartile range {IQR}, 39.1%-66.7%]) than white individuals (67.1% [IQR, 51.8%-80.6%]; P < .001). Black and Hispanic individuals treated with DOACs were more likely to receive inappropriate dosing than white individuals (black patients, 61 of 394 [15.5%]; Hispanic patients, 74 of 409 [18.1%]; white patients, 1003 of 7988 [12.6%]; P = .01). One-year persistence on oral anticoagulants was the same across groups.
Conclusions and relevance: After controlling for clinical and socioeconomic factors, black individuals were less likely than white individuals to receive DOACs for atrial fibrillation, with no difference between white and Hispanic groups. When atrial fibrillation was treated, the quality of anticoagulant use was lower in black and Hispanic individuals. Identifying modifiable causes of these disparities could improve the quality of care in atrial fibrillation.
Conflict of interest statement
Figures
Comment in
-
Cardiovascular Disease Disparities: The Gap Remains.JAMA Cardiol. 2018 Dec 1;3(12):1183. doi: 10.1001/jamacardio.2018.4040. JAMA Cardiol. 2018. PMID: 30484829 No abstract available.
References
-
- Go AS, Hylek EM, Phillips KA, et al. . Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285(18):2370-2375. doi:10.1001/jama.285.18.2370 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
