

Can we reduce ischemic cholangiopathy rates in donation after cardiac death liver transplantation after 10 years of practice? Canadian single-centre experience
- PMID: 30484989
- PMCID: PMC6351268
- DOI: 10.503/cjs.012017
Can we reduce ischemic cholangiopathy rates in donation after cardiac death liver transplantation after 10 years of practice? Canadian single-centre experience
Abstract
Background: Outcomes in liver transplantation with organs obtained via donation after cardiocirculatory death (DCD) have been suboptimal compared to donation after brain death, attributed mainly to the high incidence of ischemic cholangiopathy (IC). We evaluated the effect of a 10-year learning curve on IC rates among DCD liver graft recipients at a single centre.
Methods: We analyzed all DCD liver transplantation procedures from July 2006 to July 2016. Patients were grouped into early (July 2006 to June 2011) and late (July 2011 to July 2016) eras. Those with less than 6 months of follow-up were excluded. Primary outcomes were IC incidence and IC-free survival rate.
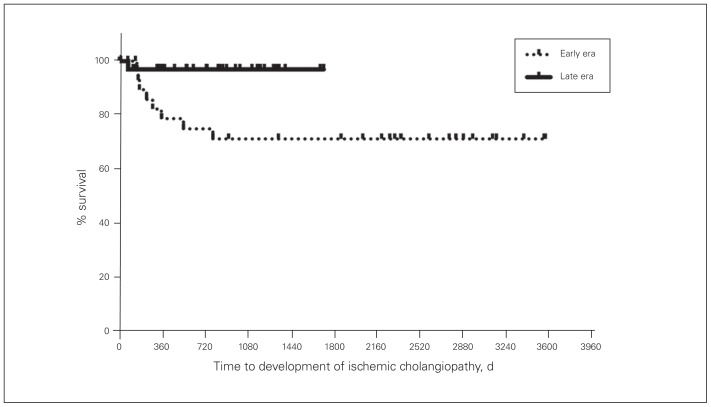
Results: Among the 73 DCD liver transplantation procedures performed, 70 recipients fulfilled the selection criteria, 32 in the early era and 38 in the late era. Biliary complications were diagnosed in 19 recipients (27%). Ischemic cholangiopathy was observed in 8 patients (25%) in the early era and 1 patient (3%) in the late era (p = 0.005). The IC-free survival rate was higher in the late era than the early era (98% v. 79%, p = 0.01). The warm ischemia time (27 v. 24 min, p = 0.049) and functional warm ischemia time (21 v. 17 min, p = 0.002) were significantly lower in the late era than the early era.
Conclusion: We found a significant reduction in IC rates and improvement in ICfree survival among DCD liver transplantation recipients after a learning curve period that was marked by more judicious donor selection with shorter procurement times.
Contexte: L’issue des greffes de foie suite à un don d’organe après décès cardiocirculatoire (DDC) a été sous-optimale comparativement aux dons suivant la mort cérébrale. Cela serait surtout attribuable à une forte incidence de cholangiopathie ischémique (CI). Nous avons évalué l’effet d’une courbe d’apprentissage échelonnée sur 10 ans sur les taux de CI chez des receveurs de greffe de foie après DDC dans un seul centre.
Méthodes: Nous avons analysé toutes les greffes de foie consécutives à des DDC entre juillet 2006 et juillet 2016. Les patients ont été regroupés en 2 époques, la première, de juillet 2006 à juin 2011, et la seconde, de juillet 2011 à juillet 2016. Ceux pour lesquels on disposait de moins de 6 mois de suivi ont été exclus. Les paramètres principaux étaient l’incidence de CI et le taux de survie sans CI.
Résultats: Parmi les 73 greffes de foie par suite de DDC, 70 receveurs répondaient aux critères de sélection, 32 pour la première époque et 38 pour la seconde époque. Des complications biliaires ont été diagnostiquées chez 19 receveurs (27 %). La cholangiopathie ischémique a été observée chez 8 patients (25 %) de la première époque et 1 patient (3 %) de la seconde (p = 0,005). Le taux de survie sans CI a été plus élevé pendant la seconde époque que pendant la première (98 % c. 79 %, p = 0,01). Le temps d’ischémie chaude (27 minutes c. 24, p = 0,049) et le temps d’ischémie chaude fonctionnelle (21 minutes c. 17, p = 0,002) ont été significativement plus courts durant la seconde époque que durant la première.
Conclusion: Nous avons observé une réduction significative des taux de CI et une amélioration de la survie sans CI chez les receveurs de greffes de foie par DDC après une courbe d’apprentissage qui a été marquée par une sélection plus judicieuse des donneurs et des délais d’obtention plus courts.
© 2019 Joule Inc. or its licensors
Conflict of interest statement
None declared.
Figures
References
-
- Mathur AK, Heimbach J, Steffick DE, et al. Donation after cardiac death liver transplantation: predictors of outcome. Am J Transplant. 2010;10:2512–9. - PubMed
-
- Busuttil RW, editor. Transplantation of the liver. 3rd ed. Philadelphia: Elsevier Saunders; 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical