

Underdetection and Undertreatment of Dyspnea in Critically Ill Patients
- PMID: 30485121
- PMCID: PMC6543712
- DOI: 10.1164/rccm.201805-0996OC
Underdetection and Undertreatment of Dyspnea in Critically Ill Patients
Abstract
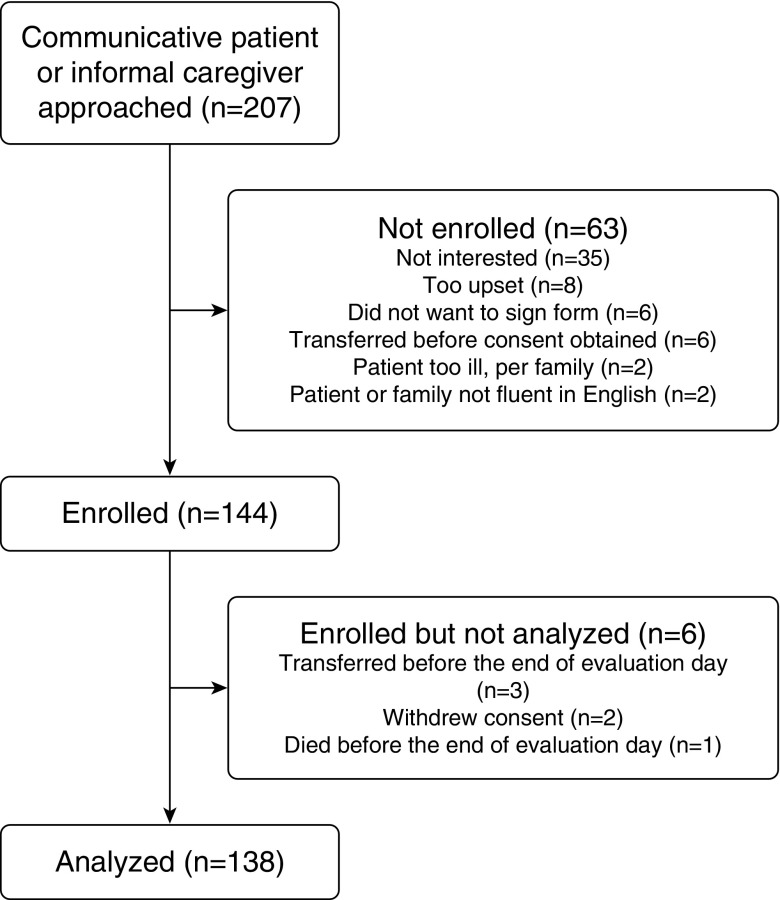
Rationale: Dyspnea is a common and distressing physical symptom among patients in the ICU and may be underdetected and undertreated. Objectives: To determine the frequency of dyspnea relative to pain, the accuracy of nurses and personal caregiver dyspnea ratings relative to patient-reported dyspnea, and the relationship between nurse-detected dyspnea and treatment. Methods: This was an observational study of patients (n = 138) hospitalized in a medical ICU (MICU). Nurses and patients' personal caregivers at the bedside reported on their perception of patients' symptoms. Measurements and Main Results: Dyspnea was assessed by patients, caregivers, and nurses with a numerical rating scale. Across all three raters, the frequency of moderate to severe dyspnea was similar or greater than that of pain (P < 0.05 for caregiver and nurse ratings). Personal caregivers' ratings of dyspnea had substantial agreement with patient ratings (κ = 0.65, P < 0.001), but nurses' ratings were not significantly related to patient ratings (κ = 0.19, P = 0.39). Nurse detection of moderate to severe pain was significantly associated with opioid treatment (odds ratio, 2.70; 95% confidence interval, 1.10-6.60; P = 0.03); however, nurse detection of moderate to severe dyspnea was not significantly associated with any assessed treatment. Conclusions: Dyspnea was reported at least as frequently as pain among the sampled MICU patients. Personal caregivers had good agreement with patient reports of moderate to severe dyspnea. However, even when detected by nurses, dyspnea appeared to be undertreated. These findings suggest the need for improved detection and treatment of dyspnea in the MICU.
Keywords: critical care; dyspnea; palliative care; symptom assessment; symptom management.
Comment in
-
Respiratory Suffering in the ICU: Time for Our Next Great Cause.Am J Respir Crit Care Med. 2019 Jun 1;199(11):1302-1304. doi: 10.1164/rccm.201812-2248ED. Am J Respir Crit Care Med. 2019. PMID: 30562045 Free PMC article. No abstract available.
References
-
- Campbell ML. Caring for dying patients in the intensive care unit: managing pain, dyspnea, anxiety, delirium, and death rattle. AACN Adv Crit Care. 2015;26:110–120. - PubMed
-
- Puntillo K, Nelson JE, Weissman D, Curtis R, Weiss S, Frontera J, et al. Advisory Board of the Improving Palliative Care in the ICU (IPAL-ICU) Project. Palliative care in the ICU: relief of pain, dyspnea, and thirst–a report from the IPAL-ICU Advisory Board. Intensive Care Med. 2014;40:235–248. - PMC - PubMed
-
- Qaseem A, Snow V, Shekelle P, Casey DE, Jr, Cross JT, Jr, Owens DK, et al. Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Evidence-based interventions to improve the palliative care of pain, dyspnea, and depression at the end of life: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2008;148:141–146. - PubMed
-
- Chanques G, Jaber S, Barbotte E, Violet S, Sebbane M, Perrigault PF, et al. Impact of systematic evaluation of pain and agitation in an intensive care unit. Crit Care Med. 2006;34:1691–1699. - PubMed
-
- Parshall MB, Schwartzstein RM, Adams L, Banzett RB, Manning HL, Bourbeau J, et al. American Thoracic Society Committee on Dyspnea. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185:435–452. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
