

Spindle cell oncocytoma of the pituitary gland
- PMID: 30485213
- PMCID: PMC6486883
- DOI: 10.3171/2018.4.JNS18211
Spindle cell oncocytoma of the pituitary gland
Abstract
Objective: The authors report the diagnosis, management, and outcomes of 6 cases of spindle cell oncocytoma (SCO) in an effort to guide clinical diagnosis and management of these uncommon lesions.
Methods: This study is a retrospective review of cases involving adult patients who underwent resection of pituitary lesions at the authors' institutions between January 2000 and October 2017. The authors identified patients with histopathological confirmation of SCO and collected clinical data, including preoperative, perioperative, and postoperative management, complications, and outcomes.
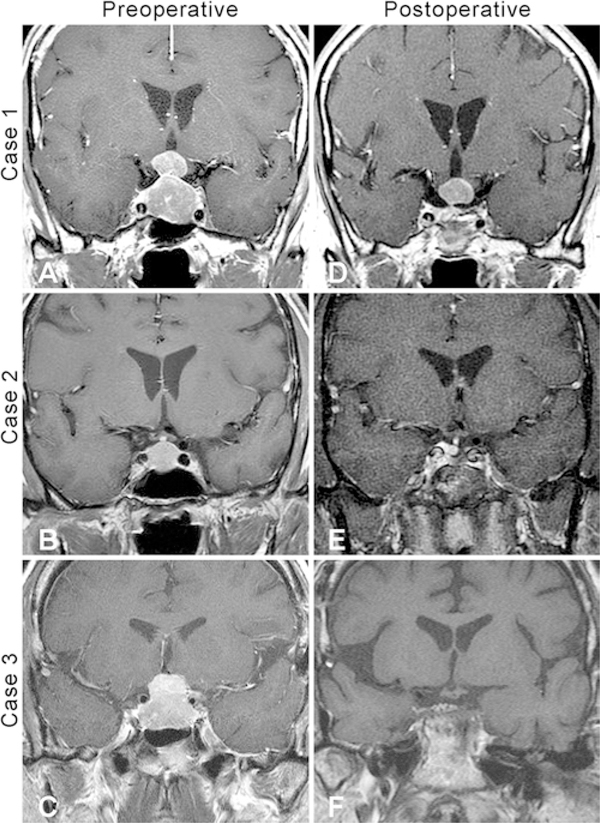
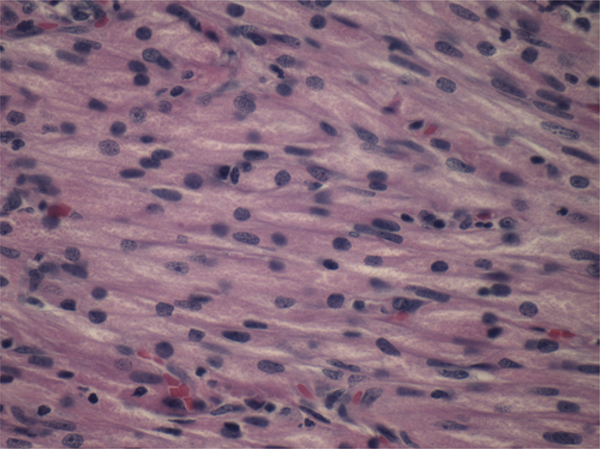
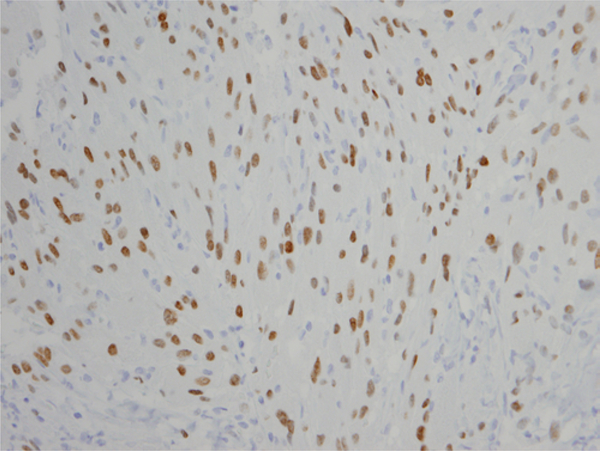
Results: Six patients with SCO were identified. Clinical findings at initial presentation included visual disturbances, dizziness, and headache. All patients underwent resection. Four resections were initially performed by the transsphenoidal approach, and 2 resections were performed by craniotomy at an outside institution with subsequent transsphenoidal reoperations. Neither necrosis nor increased mitotic activity was seen in the tumor samples. All samples stained positive for S100 protein and thyroid transcription factor 1 and negative for glial fibrillary acidic protein and pituitary hormones. Five of the samples stained positive for epithelial membrane antigen. The average MIB-1 index was 8.3% (range 2-17). Postoperatively, 3 of the 6 patients received further treatment for progression of residual tumor or for recurrence, 2 have stable residual tumor, and 1 has had no recurrence after gross-total resection. Two patients developed postoperative complications of transient sixth cranial nerve palsy and diplopia. There were no other complications.
Conclusions: SCO poses both a diagnostic and therapeutic challenge. These tumors are often initially misdiagnosed as nonfunctional pituitary adenomas because of their sellar location and nonspecific symptomatology. Postoperatively, SCO must also be distinguished from other neoplasms of the posterior pituitary gland through histopathological examination. Resection of SCO can be challenging, given its highly vascular and adherent nature. Long-term follow-up is critical, as the tumor is associated with higher recurrence and progression rates compared to other benign neoplasms of the sella.
Keywords: CN = cranial nerve; CNS = central nervous system; EMA = epithelial membrane antigen; GFAP = glial fibrillary acidic protein; GTR = gross-total resection; OSH = outside hospital; S100 = S100 protein; SCO = spindle cell oncocytoma; TS = transsphenoidal; TTF-1 = thyroid transcription factor 1; WHO = World Health Organization; neurosurgery; pituitary surgery; spindle cell oncocytoma; transsphenoidal.
Conflict of interest statement
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
-
- Alexandrescu S, Brown RE, Tandon N, Bhattacharjee MB: Neuron precursor features of spindle cell oncocytoma of adenohypophysis. Ann Clin Lab Sci 42:123–129, 2012 - PubMed
-
- Billeci D, Marton E, Giordan E, Carraro V, Ronzon M, Rossi S: Spindle cell oncocytoma: report of two cases with massive bleeding and review of the literature. J Clin Neurosci 39:39–44, 2017 - PubMed
-
- Borges MT, Lillehei KO, Kleinschmidt-DeMasters BK: Spindle cell oncocytoma with late recurrence and unique neuroimaging characteristics due to recurrent subclinical intratumoral bleeding. J Neurooncol 101:145–154, 2011 - PubMed
-
- Borota OC, Scheithauer BW, Fougner SL, Hald JK, RammPettersen J, Bollerslev J: Spindle cell oncocytoma of the adenohypophysis: report of a case with marked cellular atypia and recurrence despite adjuvant treatment. Clin Neuropathol 28:91–95, 2009 - PubMed
-
- Coiré CI, Horvath E, Smyth HS, Kovacs K: Rapidly recurring folliculostellate cell tumor of the adenohypophysis with the morphology of a spindle cell oncocytoma: case report with electron microscopic studies. Clin Neuropathol 28:303–308, 2009 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
