

How to Treat Chronic Subdural Hematoma? Past and Now
- PMID: 30486622
- PMCID: PMC6411568
- DOI: 10.3340/jkns.2018.0156
How to Treat Chronic Subdural Hematoma? Past and Now
Abstract
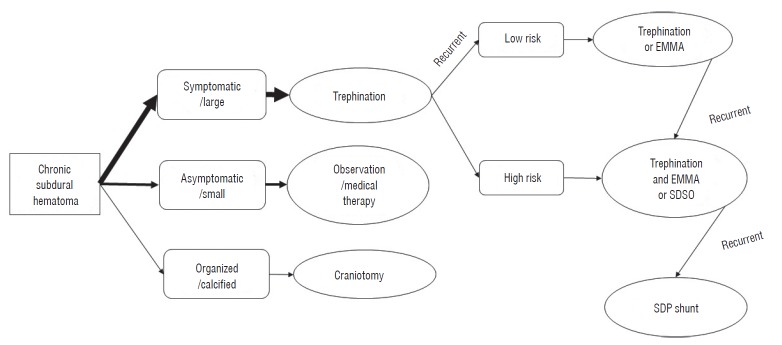
Treatment of chronic subdural hematoma (CSDH) is relatively straightforward, however, there is still some debate regarding the best strategy for treatment. The most practical recommendations of up to date were identified by a review of literature. The author reviewed the literature on CSDH management from the past to now to identify the best methods. Till 1970s, craniotomy was the most commonly used method. Burr hole (BH) became the most preferred method from 1980s. In 1977, twist drill (TD) craniostomy was introduced. Closed system drainage after a BH or a TD became the most frequently used surgical method. Although nonsurgical treatment is often successful, trephination has more advantages, such as rapid resolution of the symptoms and short period of hospitalization. Nonsurgical treatment is possible in asymptomatic patients with a small CSDH. For the symptomatic patients with CSDH, trephination is the treatment of choice, either by BH or TD. In gray zone between surgery and medical treatment, shared decision making can be an ideal approach. For the recurrent CSDHs, repeated trephination is still effective for patients with a low risk of recurrence. If the risk of recurrence is high, additional management would be helpful. For the refractory CSDHs, it is necessary to obliterate the subdural space.
Keywords: Conservative treatment; Craniocerebral trauma; Craniotomy; Hematoma, Subdural, Chronic; Recurrence; Trephining.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Which surgical procedure is effective for refractory chronic subdural hematoma? Analysis of our surgical procedures and literature review.J Clin Neurosci. 2018 Mar;49:40-47. doi: 10.1016/j.jocn.2017.11.009. Epub 2017 Dec 20. J Clin Neurosci. 2018. PMID: 29274740 Review.
-
Remote Hemorrhage after Burr Hole Drainage of Chronic Subdural Hematoma.Korean J Neurotrauma. 2017 Oct;13(2):144-148. doi: 10.13004/kjnt.2017.13.2.144. Epub 2017 Oct 31. Korean J Neurotrauma. 2017. PMID: 29201850 Free PMC article.
-
Outcome of contemporary surgery for chronic subdural haematoma: evidence based review.J Neurol Neurosurg Psychiatry. 2003 Jul;74(7):937-43. doi: 10.1136/jnnp.74.7.937. J Neurol Neurosurg Psychiatry. 2003. PMID: 12810784 Free PMC article.
-
Intracatheter Tissue Plasminogen Activator for Chronic Subdural Hematomas after Failed Bedside Twist Drill Craniostomy: A Retrospective Review.Cureus. 2019 Dec 26;11(12):e6472. doi: 10.7759/cureus.6472. Cureus. 2019. PMID: 32025399 Free PMC article.
-
Chronic subdural hematoma.Asian J Neurosurg. 2016 Oct-Dec;11(4):330-342. doi: 10.4103/1793-5482.145102. Asian J Neurosurg. 2016. PMID: 27695533 Free PMC article. Review.
Cited by
-
Middle meningeal artery embolisation: The review of a new treatment for chronic subdural hematomas.Surg Neurol Int. 2023 Feb 24;14:66. doi: 10.25259/SNI_1096_2022. eCollection 2023. Surg Neurol Int. 2023. PMID: 36895214 Free PMC article. Review.
-
Middle Meningeal Artery Embolization in the Management of Chronic Subdural Hematoma: a Comprehensive Review of Current Literature.Curr Neurol Neurosci Rep. 2023 Apr;23(4):109-119. doi: 10.1007/s11910-023-01262-6. Epub 2023 Apr 11. Curr Neurol Neurosci Rep. 2023. PMID: 37037979 Review.
-
Role of Adjunctive Tranexamic Acid in Facilitating Resolution of Chronic Subdural Hematoma after Surgery.J Korean Neurosurg Soc. 2023 Jul;66(4):446-455. doi: 10.3340/jkns.2022.0200. Epub 2022 Nov 3. J Korean Neurosurg Soc. 2023. PMID: 36325752 Free PMC article.
-
Intraoperative hematoma volume can predict chronic subdural hematoma recurrence.Surg Neurol Int. 2021 May 25;12:232. doi: 10.25259/SNI_97_2021. eCollection 2021. Surg Neurol Int. 2021. PMID: 34221563 Free PMC article.
-
Adjunct Middle Meningeal Artery Embolization Versus Surgery for Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis.Neurosurg Rev. 2024 Nov 28;47(1):876. doi: 10.1007/s10143-024-03107-3. Neurosurg Rev. 2024. PMID: 39607623
References
-
- Alcalá-Cerra G, Young AM, Moscote-Salazar LR, Paternina-Caicedo Á. Efficacy and safety of subdural drains after burr-hole evacuation of chronic subdural hematomas: systematic review and meta-analysis of randomized controlled trials. World Neurosurg. 2014;82:1148–1157. - PubMed
-
- Almenawer SA, Farrokhyar F, Hong C, Alhazzani W, Manoranjan B, Yarascavitch B, et al. Chronic subdural hematoma management: a systematic review and meta-analysis of 34,829 patients. Ann Surg. 2014;259:449–457. - PubMed
-
- Ambrosetto C. Post-traumatic subdural hematoma. Further observations on nonsurgical treatment. Arch Neurol. 1962;6:287–292. - PubMed
-
- Aoki N. Chronic subdural hematoma in infancy. Clinical analysis of 30 cases in the CT era. J Neurosurg. 1990;73:201–205. - PubMed
-
- Arginteanu MS, Byun H, King W. Treatment of a recurrent subdural hematoma using urokinase. J Neurotrauma. 1999;16:1235–1239. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
