

Health-care utilization for headache disorders in Nepal: a population-based door-to-door survey
- PMID: 30486777
- PMCID: PMC6755598
- DOI: 10.1186/s10194-018-0942-3
Health-care utilization for headache disorders in Nepal: a population-based door-to-door survey
Abstract
Background: Headache disorders are an important global public-health problem, but under-diagnosed, undertreated and under-prioritized. Deficiencies in health care for headache, present everywhere, are likely to be greater in poorly-resourced countries. This study reports on health-care utilization for headache in Nepal, a low-income country with high headache burden.
Methods: We took data from a cross-sectional, nationwide population-based door-to-door survey, with multistage cluster random sampling. Face-to-face structured interviews included enquiry into consultations with professional health-care providers (HCPs), and investigations and treatments for headache. Analysis included associations with sociodemographic variables and indices of symptom severity.
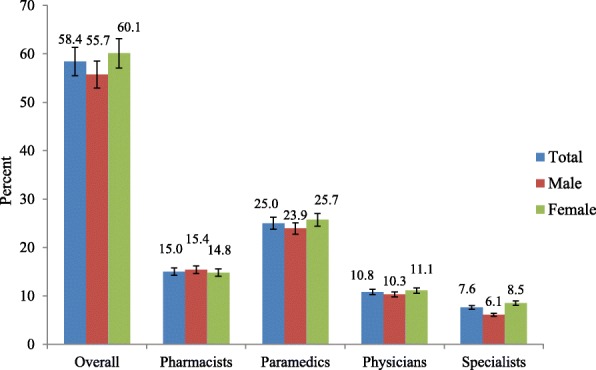
Results: Of 2100 participants, 1794 reported headache during the preceding year (mean age 36.1 ± 12.6 years; male/female ratio 1:1.6). Of these, 58.4% (95% CI: 56.1-60.7%) had consulted at least once in the year with HCPs at any level, most commonly (25.0%) paramedical; 15.0% had consulted pharmacists, 10.8% general physicians and 7.6% specialists (of any type). Participants with probable medication-overuse headache consulted most (87.0%), followed by those with migraine (67.2%) and those with tension-type headache (48.6%; p < 0.001). A minority (11.9%) were investigated, mostly (8.9%) by eye tests. Half (50.8%) had used conventional medications for headache in the preceding month, paracetamol being by far the most common (38.0%), and 10.3% had used herbal therapies. Consultation was positively associated with rural habitation (AOR = 1.5; p < 0.001). Proportions consulting increased in line with all indices of symptom severity.
Conclusions: Although over half of participants with headache had consulted professional HCPs, this reflects demand, not quality of care. Although 7.6% had seen specialists, very few would have been headache specialists in any sense of this term. High persistent burden, with only half of participants with headache using conventional medications, and these not best chosen, suggests these consultations fell far short of meeting need. Health policy in Nepal should recognise this, since the consequences otherwise are costly: lost health, diminished productivity and damaged national economy. On a positive note, the proportions consulting suggest that capacity exists at multiple levels within the Nepalese health system. With this to build upon, structured headache services in line with international recommendations appear achievable in Nepal. Educational programmes are the essential requirement.
Keywords: Global campaign against headache; Headache disorders; Health-care utilization; Medical consultation; Nepal; Population-based study; Quality of care; Structured headache services.
Conflict of interest statement
TJS is a Director and Trustee of
Figures
Similar articles
-
The burden of headache disorders in Nepal: estimates from a population-based survey.J Headache Pain. 2015;17:3. doi: 10.1186/s10194-016-0594-0. Epub 2016 Jan 25. J Headache Pain. 2015. PMID: 26810487 Free PMC article.
-
The burden of headache disorders in Ethiopia: national estimates from a population-based door-to-door survey.J Headache Pain. 2017 Dec;18(1):58. doi: 10.1186/s10194-017-0765-7. Epub 2017 May 25. J Headache Pain. 2017. PMID: 28547735 Free PMC article.
-
Prevalence and burden of headache disorders in Lithuania and their public-health and policy implications: a population-based study within the Eurolight Project.J Headache Pain. 2017 Dec;18(1):53. doi: 10.1186/s10194-017-0759-5. Epub 2017 May 4. J Headache Pain. 2017. PMID: 28474253 Free PMC article.
-
The methodology of population surveys of headache prevalence, burden and cost: principles and recommendations from the Global Campaign against Headache.J Headache Pain. 2014 Jan 27;15(1):5. doi: 10.1186/1129-2377-15-5. J Headache Pain. 2014. PMID: 24467862 Free PMC article. Review.
-
Rethinking headache as a global public health case model for reaching the SDG 3 HEALTH by 2030.J Headache Pain. 2023 Oct 27;24(1):140. doi: 10.1186/s10194-023-01666-2. J Headache Pain. 2023. PMID: 37884869 Free PMC article. Review.
Cited by
-
Structured headache services as the solution to the ill-health burden of headache: 1. Rationale and description.J Headache Pain. 2021 Jul 21;22(1):78. doi: 10.1186/s10194-021-01265-z. J Headache Pain. 2021. PMID: 34289806 Free PMC article.
-
The Global Campaign turns 18: a brief review of its activities and achievements.J Headache Pain. 2022 Apr 21;23(1):49. doi: 10.1186/s10194-022-01420-0. J Headache Pain. 2022. PMID: 35448941 Free PMC article. Review.
-
Morbidities, health problems, health care seeking and utilization behaviour among elderly residing on urban areas of eastern Nepal: A cross-sectional study.PLoS One. 2022 Sep 7;17(9):e0273101. doi: 10.1371/journal.pone.0273101. eCollection 2022. PLoS One. 2022. PMID: 36070314 Free PMC article.
-
The HARDSHIP databases: a forthcoming free good from the Global Campaign against Headache.J Headache Pain. 2023 Mar 6;24(1):21. doi: 10.1186/s10194-023-01554-9. J Headache Pain. 2023. PMID: 36879195 Free PMC article.
References
-
- World Health Organization and Lifting The Burden . Atlas of headache disorders and resources in the world 2011. Geneva: WHO; 2011.
-
- Linde M, Gustavsson A, Stovner LJ, Steiner TJ, Barre J, Katsarava Z, Lainez JM, Lampl C, Lanteri-Minet M, Rastenyte D, Ruiz de la Torre E, Tassorelli C, Andree C. The cost of headache disorders in Europe: the Eurolight project. Eur J Neurol. 2012;19(5):703–711. doi: 10.1111/j.1468-1331.2011.03612.x. - DOI - PubMed
-
- Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, Carter A, Casey DC, Charlson FJ, Chen AZ, Coggeshall M, Cornaby L, Dandona L, Dicker DJ, Dilegge T, Erskine HE, Ferrari AJ, Fitzmaurice C, Fleming T, Forouzanfar MH, Fullman N, Gething PW, Goldberg EM, Graetz N, Haagsma JA, Johnson CO, Kassebaum NJ, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602. doi: 10.1016/s0140-6736(16)31678-6. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
