

De-implementation of low value castration for men with prostate cancer: protocol for a theory-based, mixed methods approach to minimizing low value androgen deprivation therapy (DeADT)
- PMID: 30486836
- PMCID: PMC6262964
- DOI: 10.1186/s13012-018-0833-7
De-implementation of low value castration for men with prostate cancer: protocol for a theory-based, mixed methods approach to minimizing low value androgen deprivation therapy (DeADT)
Abstract
Background: Men with prostate cancer are often castrated with long-acting injectable drugs termed androgen deprivation therapy (ADT). Although many benefit, ADT is also used in patients with little or nothing to gain. The best ways to stop this practice are unknown, and range from blunt pharmacy restrictions to informed decision-making. This study will refine and pilot two different de-implementation strategies for reducing ADT use among those unlikely to benefit in preparation for a comparative effectiveness trial.
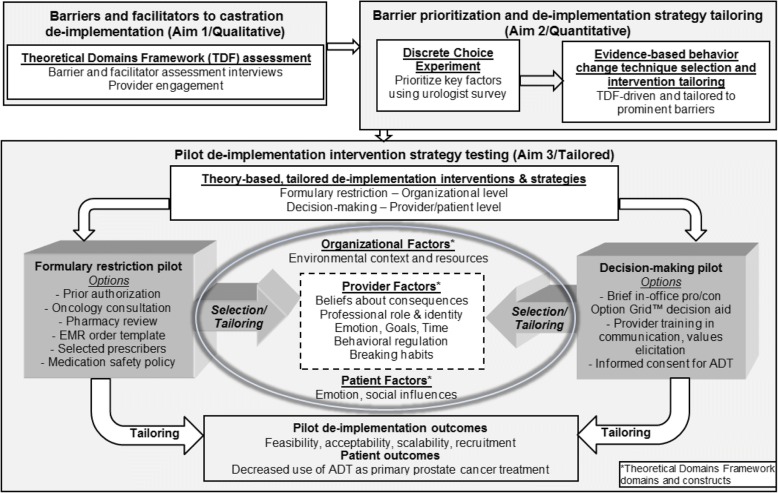
Methods/design: This innovative mixed methods research program has three aims. Aim 1: To assess preferences and barriers for de-implementation of chemical castration in prostate cancer. Guided by the theoretical domains framework (TDF), urologists and patients from facilities with the highest and lowest castration rates across the VA will be interviewed to identify key preferences and de-implementation barriers for reducing castration as prostate cancer treatment. This qualitative work will inform Aim 2 while gathering rich information for two proposed pilot intervention strategies. Aim 2: To use a discrete choice experiment (DCE), a novel barrier prioritization approach, for de-implementation strategy tailoring. The investigators will conduct national surveys of urologists to prioritize key barriers identified in Aim 1 for stopping incident castration as localized prostate cancer treatment using a DCE experiment design. These quantitative results will identify the most important barriers to be addressed through tailoring of two pilot de-implementation strategies in preparation for Aim 3 piloting. Aim 3: To pilot two tailored de-implementation strategies to reduce castration as localized prostate cancer treatment. Building on findings from Aims 1 and 2, two de-implementation strategies will be piloted. One strategy will focus on formulary restriction at the organizational level and the other on physician/patient informed decision-making at different facilities. Outcomes will include acceptability, feasibility, and scalability in preparation for an effectiveness trial comparing these two widely varying de-implementation strategies.
Discussion: Our innovative approach to de-implementation strategy development is directly aligned with state-of-the-art complex implementation intervention development and implementation science. This work will broadly advance de-implementation science for low value cancer care, and foster participation in our de-implementation evaluation trial by addressing barriers, facilitators, and concerns through pilot tailoring.
Trial registration: ClinicalTrials.gov Identifier: NCT03579680 , First Posted July 6, 2018.
Keywords: Androgen deprivation therapy (ADT); Behavior change; Castration; Choosing wisely; De-implementation; Decision-making; Discrete choice; Formulary restriction; Implementation science; Intervention; Low value care; Stakeholder.
Conflict of interest statement
Ethics approval and consent to participate
This study has been approved by the VA Ann Arbor Healthcare System IRB (IRB-2017-1047) and the University of Michigan IRB (HUM00133932). As this study is conducted solely by phone and by mail and is considered minimal risk, a waiver of documentation of signed informed consent and HIPAA Authorization was approved. Verbal informed consent is obtained for all patients participating in the research. Further information and documentation on IRB approval is available upon request.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests. Dr. Skolarus is a prostate cancer survivorship author for UpToDate™.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Unpacking overuse of androgen deprivation therapy for prostate cancer to inform de-implementation strategies.Implement Sci Commun. 2024 Apr 9;5(1):37. doi: 10.1186/s43058-024-00576-x. Implement Sci Commun. 2024. PMID: 38594740 Free PMC article.
-
Learning from the "tail end" of de-implementation: the case of chemical castration for localized prostate cancer.Implement Sci Commun. 2021 Oct 28;2(1):124. doi: 10.1186/s43058-021-00224-8. Implement Sci Commun. 2021. PMID: 34711274 Free PMC article.
-
The Individualized Diet and Exercise Adherence Pilot Trial (IDEA-P) in prostate cancer patients undergoing androgen deprivation therapy: study protocol for a randomized controlled trial.Trials. 2014 Sep 9;15:354. doi: 10.1186/1745-6215-15-354. Trials. 2014. PMID: 25199619 Free PMC article. Clinical Trial.
-
Intermittent androgen-deprivation therapy in prostate cancer: a critical review focused on phase 3 trials.Eur Urol. 2013 Nov;64(5):722-30. doi: 10.1016/j.eururo.2013.04.020. Epub 2013 Apr 19. Eur Urol. 2013. PMID: 23628492 Review.
-
Optimizing the role of androgen deprivation therapy in advanced prostate cancer: Challenges beyond the guidelines.Prostate. 2020 May;80(6):527-544. doi: 10.1002/pros.23967. Epub 2020 Mar 4. Prostate. 2020. PMID: 32130741 Free PMC article. Review.
Cited by
-
Unpacking overuse of androgen deprivation therapy for prostate cancer to inform de-implementation strategies.Implement Sci Commun. 2024 Apr 9;5(1):37. doi: 10.1186/s43058-024-00576-x. Implement Sci Commun. 2024. PMID: 38594740 Free PMC article.
-
Applying the behavior change wheel to design de-implementation strategies to reduce low-value statin prescription in primary prevention of cardiovascular disease in primary care.Front Med (Lausanne). 2022 Oct 13;9:967887. doi: 10.3389/fmed.2022.967887. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36314033 Free PMC article.
-
A scoping review of de-implementation frameworks and models.Implement Sci. 2021 Nov 24;16(1):100. doi: 10.1186/s13012-021-01173-5. Implement Sci. 2021. PMID: 34819122 Free PMC article.
-
Reducing the frequency of hand hygiene to maintain skin integrity among nurses in the growing care unit: A pilot study.Fujita Med J. 2025 Aug;11(3):135-141. doi: 10.20407/fmj.2024-029. Epub 2025 Apr 17. Fujita Med J. 2025. PMID: 40777146 Free PMC article.
-
Creation of a theoretically rooted workbook to support implementers in the practice of knowledge translation.Implement Sci Commun. 2023 Aug 18;4(1):99. doi: 10.1186/s43058-023-00480-w. Implement Sci Commun. 2023. PMID: 37596659 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
