

"Sometimes it is difficult for us to stand up and change this": an analysis of power within priority-setting for health following devolution in Kenya
- PMID: 30486867
- PMCID: PMC6264027
- DOI: 10.1186/s12913-018-3706-5
"Sometimes it is difficult for us to stand up and change this": an analysis of power within priority-setting for health following devolution in Kenya
Abstract
Background: Practices of power lie at the heart of policy processes. In both devolution and priority-setting, actors seek to exert power through influence and control over material, human, intellectual and financial resources. Priority-setting arises as a consequence of the needs and demand exceeding the resources available, requiring some means of choosing between competing demands. This paper examines the use of power within priority-setting processes for healthcare resources at sub-national level, following devolution in Kenya.
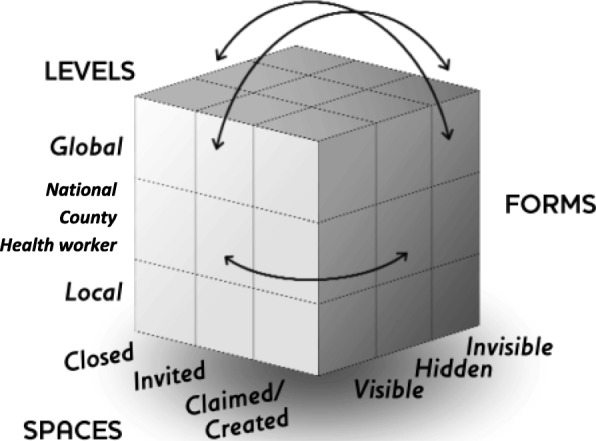
Methods: We interviewed 14 national level key informants and 255 purposively selected respondents from across the health system in ten counties. These qualitative data were supplemented by 14 focus group discussions (FGD) involving 146 community members in two counties. We conducted a power analysis using Gaventa's power cube and Veneklasen's expressions of power to interpret our findings.
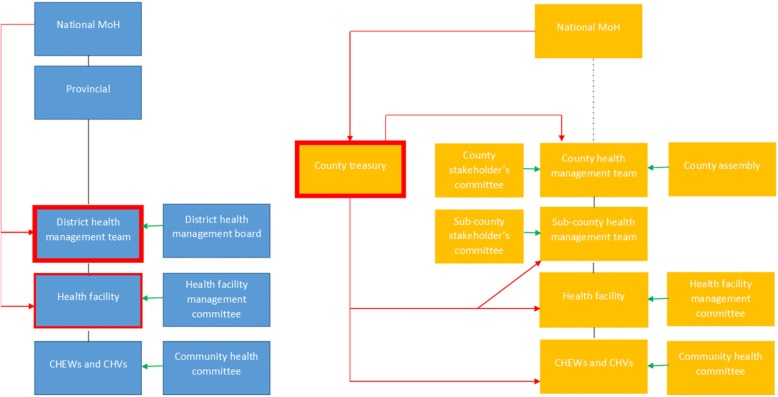
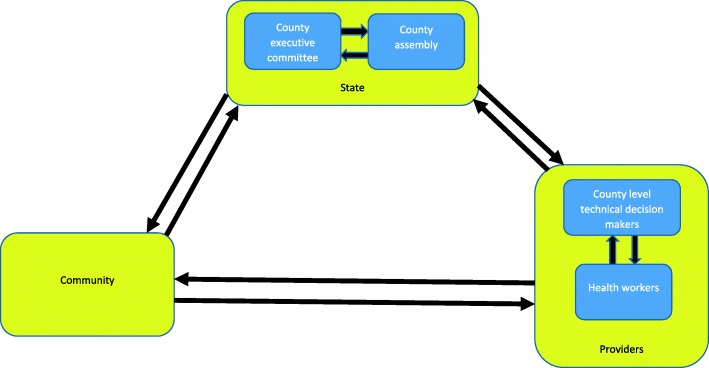
Results: We found Kenya's transition towards devolution is transforming the former centralised balance of power, leading to greater ability for influence at the county level, reduced power at national and sub-county (district) levels, and limited change at community level. Within these changing power structures, politicians are felt to play a greater role in priority-setting for health. The interfaces and tensions between politicians, health service providers and the community has at times been felt to undermine health related technical priorities. Underlying social structures and discriminatory practices generally continue unchanged, leading to the continued exclusion of the most vulnerable from priority-setting processes.
Conclusions: Power analysis of priority-setting at county level after devolution in Kenya highlights the need for stronger institutional structures, processes and norms to reduce the power imbalances between decision-making actors and to enable community participation.
Keywords: Devolution; Kenya; Power; Priority-setting.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was received from Kenya Medical Research Institute (KEMRI) and Liverpool School of Tropical Medicine, with research permit from National Commission for Science Technology and Innovation (NACOSTI). Written informed consent was sought from and signed by all interviewed respondents.
Consent for publication
The manuscript has anonymised information to ensure confidentiality.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Priority setting for health in the context of devolution in Kenya: implications for health equity and community-based primary care.Health Policy Plan. 2018 Jul 1;33(6):729-742. doi: 10.1093/heapol/czy043. Health Policy Plan. 2018. PMID: 29846599 Free PMC article.
-
Tracking health sector priority setting processes and outcomes for human resources for health, five-years after political devolution: a county-level case study in Kenya.Int J Equity Health. 2020 Sep 21;19(1):165. doi: 10.1186/s12939-020-01284-3. Int J Equity Health. 2020. PMID: 32958000 Free PMC article.
-
Applying an intersectionality lens to examine health for vulnerable individuals following devolution in Kenya.Int J Equity Health. 2019 Jan 30;18(1):24. doi: 10.1186/s12939-019-0917-2. Int J Equity Health. 2019. PMID: 30700299 Free PMC article.
-
Devolution of healthcare system in Kenya: progress and challenges.Public Health. 2020 Dec;189:135-140. doi: 10.1016/j.puhe.2020.10.001. Epub 2020 Nov 20. Public Health. 2020. PMID: 33227596
-
Strengthening fairness, transparency and accountability in health care priority setting at district level in Tanzania.Glob Health Action. 2011;4. doi: 10.3402/gha.v4i0.7829. Epub 2011 Nov 7. Glob Health Action. 2011. PMID: 22072991 Free PMC article. Review.
Cited by
-
Health managers' perspectives of community health committees' participation in the annual health sector planning and budgeting process in a devolved unit in Kenya: a cross-sectional study.Pan Afr Med J. 2024 Mar 20;47:124. doi: 10.11604/pamj.2024.47.124.40351. eCollection 2024. Pan Afr Med J. 2024. PMID: 38854860 Free PMC article.
-
How do decision-makers use evidence in community health policy and financing decisions? A qualitative study and conceptual framework in four African countries.Health Policy Plan. 2020 Aug 1;35(7):799-809. doi: 10.1093/heapol/czaa027. Health Policy Plan. 2020. PMID: 32516361 Free PMC article.
-
Geographic prioritisation in Kenya and Uganda: a power analysis of donor transition.BMJ Glob Health. 2023 May;8(5):e010499. doi: 10.1136/bmjgh-2022-010499. BMJ Glob Health. 2023. PMID: 37236658 Free PMC article.
-
Evaluating the effects, implementation experience and political economy of primary healthcare facility autonomy reforms within counties in Kenya: a mixed methods study protocol.BMJ Public Health. 2024 Jul;2(2):e001156. doi: 10.1136/bmjph-2024-001156. Epub 2024 Oct 15. BMJ Public Health. 2024. PMID: 39822946 Free PMC article.
-
Unmet need for primary healthcare and associated individual and household-level factors in Kenya: results from a national survey.BMJ Open. 2021 May 28;11(5):e041032. doi: 10.1136/bmjopen-2020-041032. BMJ Open. 2021. PMID: 34049900 Free PMC article.
References
-
- L. VeneKlasen, V. Miller, D. Budlender, and C. Clark, “power and empowerment,” in A New Weave of Power, People and Politics: The Action Guide for Advocacy and Citizen Participation, vol. 43, 2002, pp. 39–41.
-
- Confederation TNHS. London, UK. 2007. Priority setting : an overview the voice of NHS leadership.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
