

Post-approval upper airway stimulation predictors of treatment effectiveness in the ADHERE registry
- PMID: 30487205
- PMCID: PMC6319796
- DOI: 10.1183/13993003.01405-2018
Post-approval upper airway stimulation predictors of treatment effectiveness in the ADHERE registry
Abstract
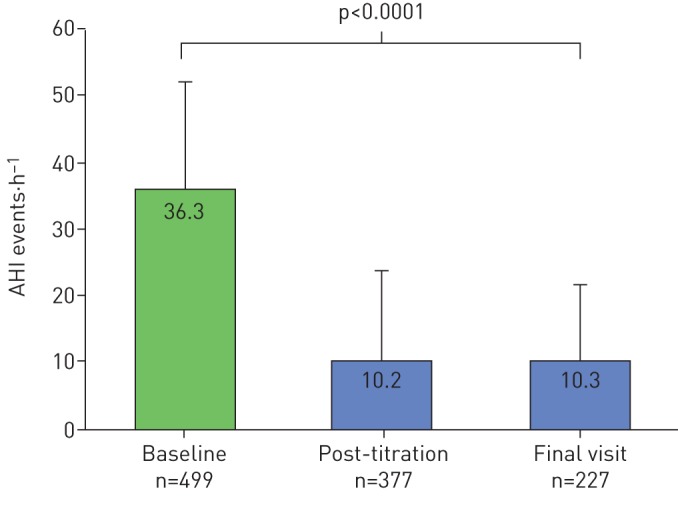
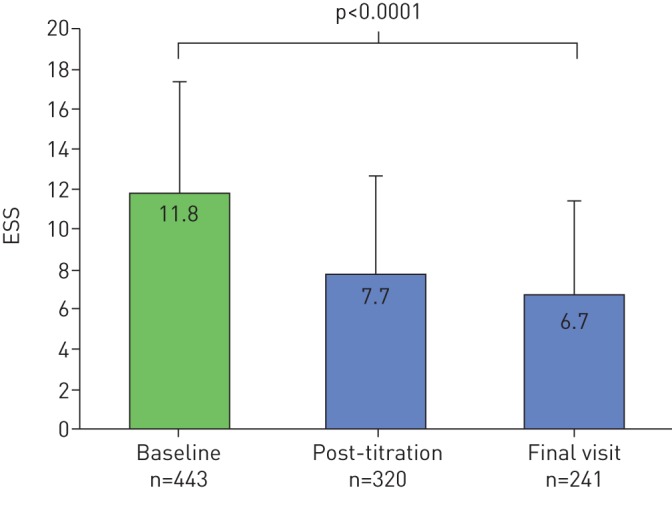
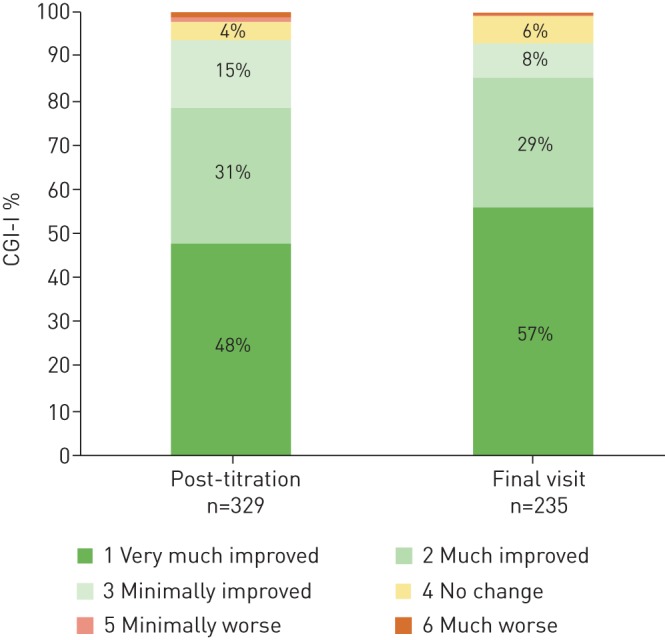
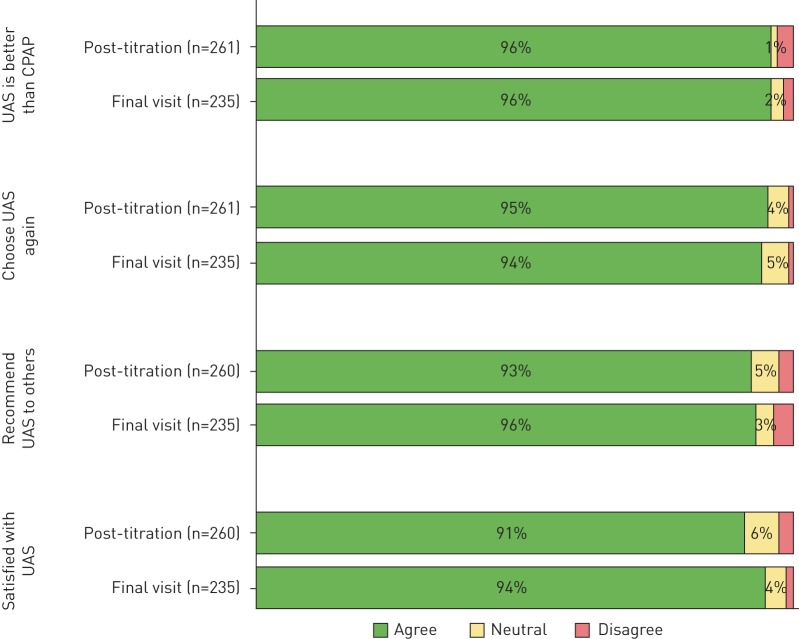
Upper airway stimulation (UAS) has been shown to reduce severity of obstructive sleep apnoea. The aim of this study was to identify predictors of UAS therapy response in an international multicentre registry.Patients who underwent UAS implantation in the United States and Germany were enrolled in an observational registry. Data collected included patient characteristics, apnoea/hypopnoea index (AHI), Epworth sleepiness scale (ESS), objective adherence, adverse events and patient satisfaction measures. Post hoc univariate and multiple logistic regression were performed to evaluate factors associated with treatment success.Between October 2016 and January 2018, 508 participants were enrolled from 14 centres. Median AHI was reduced from 34 to 7 events·h-1, median ESS reduced from 12 to 7 from baseline to final visit at 12-month post-implant. In post hoc analyses, for each 1-year increase in age, there was a 4% increase in odds of treatment success. For each 1-unit increase in body mass index (BMI), there was 9% reduced odds of treatment success. In the multivariable model, age persisted in serving as statistically significant predictor of treatment success.In a large multicentre international registry, UAS is an effective treatment option with high patient satisfaction and low adverse events. Increasing age and reduced BMI are predictors of treatment response.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: C. Heiser reports grants and personal fees from Inspire Medical Systems (Maple Grove, MN, USA), during the conduct of the study; and grants and personal fees for consultancy from Inspire Medical Systems, outside the submitted work. Conflict of interest: A. Steffen has received reimbursement of conference fees and travel and accommodation expenses, fees for preparing scientific continuing professional development or other events, funding for research he himself initiated, and fees for conducting clinical studies on related subjects from Inspire Medical Systems. Conflict of interest: M. Boon reports grants from Inspire Medical Systems, during the conduct of the study; and grants and personal fees for consultancy from Inspire Medical Systems, outside the submitted work. Conflict of interest: B. Hofauer reports personal fees from Inspire Medical Systems, during the conduct of the study. Conflict of interest: K. Doghramji reports grants from Inspire Medical Systems, during the conduct of the study; and grants and personal fees from Inspire Medical Systems, outside the submitted work. Conflict of interest: J.T. Maurer reports grants and personal fees for lectures, surgical training and consulting from Inspire Medical Systems, during the conduct of the study; and grants and personal fees for surgical training from Imthera and Revent, grants and personal fees for consultancy from Philipps and Nyxoah, and personal fees for lecturing from GlaxoSmithKline, Heinen und Löwenstein, Weinmann, Sissel Novacare, ResMed, Olympus, Neuwirth Medical and Medtronic, outside the submitted work. Conflict of interest: J.U. Sommer reports grants, personal fees and non-financial support from Inspire Medical Systems, ImThera, Regis Medical, Nyxoah, Phillips, MedEl, and personal fees from Neucomed, during the conduct of the study. Conflict of interest: R. Soose was a consultant and study investigator for Inspire Medical Systems, during the conduct of the study; and carried out advisory board and consultancy work for Galvani Bioelectronics, and was a consultant for Invicta Medical, outside the submitted work. Conflict of interest: P.J. Strollo Jr reports grants and personal fees for consultancy from Inspire Medical Systems and Jazz Pharmaceuticals, and personal fees for consultancy from Philips-Respironics and Itamar Medical, outside the submitted work. Conflict of interest: R. Schwab reports grants from Inspire Medical Systems, during the conduct of the study. Conflict of interest: E. Thaler is a consultant for Inspire Medical Systems, outside the submitted work. Conflict of interest: K. Withrow has nothing to disclose. Conflict of interest: A. Kominsky has nothing to disclose. Conflict of interest: C. Larsen has nothing to disclose. Conflict of interest: E.J. Kezirian reports grants from Inspire Medical Systems, during the conduct of the study; and equity from Nyxoah, Pillar Palatal, Cognitive Life Science, Split Rock Scientific, Gerard Scientific, Berendo Scientific and ReVENT Medical, and grants from Autonomic Technologies, outside the submitted work; and in addition, has a patent Magnap issued, a patent Endoscopic Device and System issued, a patent Head and Neck Exercise Methods pending, and a patent Airway and Airflow Factors issued. Conflict of interest: J. Hsia has nothing to disclose. Conflict of interest: S. Chia has nothing to disclose. Conflict of interest: J. Harwick has nothing to disclose. Conflict of interest: K. Strohl reports grants (as site PI for post-approval studies) from Inspire Medical Systems, during the conduct of the study; and was consultant to Sommetrics and advisor to Galvani Bioelectronics, outside the submitted work. Conflict of interest: R. Mehra reports grants (to institution, to support efforts to collect data for the ADHERE registry) from Inspire Medical Systems, during the conduct of the study; and grants from NIH, equipment for research from Philips Respironics and Resmed, personal fees from American Academy of Sleep Medicine, and royalties from Up to Date, outside the submitted work.
Figures
References
-
- Remmers JE, de Groot WJ, Sauerland EK, et al. Pathogenesis of upper airway occlusion during sleep. J Appl Physiol Respir Environ Exerc Physiol 1978; 44: 931–938. - PubMed
-
- Strohl KP, Saunders NA, Feldman NT, et al. Obstructive sleep apnea in family members. N Engl J Med 1978; 299: 969–973. - PubMed
-
- Eckert DJ. Phenotypic approaches to obstructive sleep apnoea – new pathways for targeted therapy. Sleep Med Rev 2018; 37: 45–59. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources