

Aortic stiffness in aortic stenosis assessed by cardiovascular MRI: a comparison between bicuspid and tricuspid valves
- PMID: 30488106
- PMCID: PMC6443917
- DOI: 10.1007/s00330-018-5775-6
Aortic stiffness in aortic stenosis assessed by cardiovascular MRI: a comparison between bicuspid and tricuspid valves
Abstract
Objectives: To compare aortic size and stiffness parameters on MRI between bicuspid aortic valve (BAV) and tricuspid aortic valve (TAV) patients with aortic stenosis (AS).
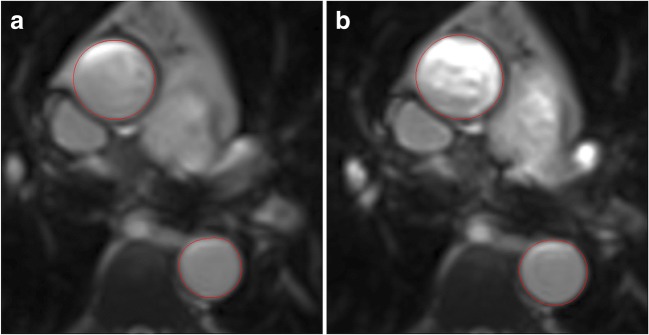
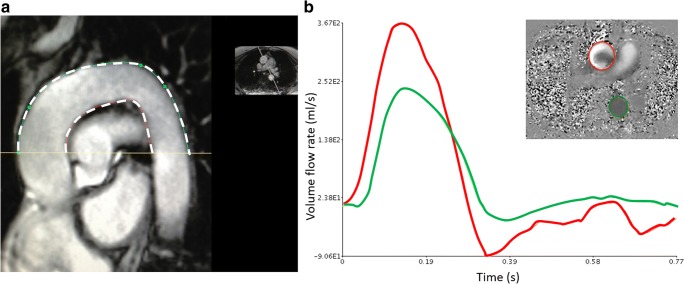
Methods: MRI was performed in 174 patients with asymptomatic moderate-severe AS (mean AVAI 0.57 ± 0.14 cm2/m2) and 23 controls on 3T scanners. Valve morphology was available/analysable in 169 patients: 63 BAV (41 type-I, 22 type-II) and 106 TAV. Aortic cross-sectional areas were measured at the level of the pulmonary artery bifurcation. The ascending and descending aorta (AA, DA) distensibility, and pulse wave velocity (PWV) around the aortic arch were calculated.
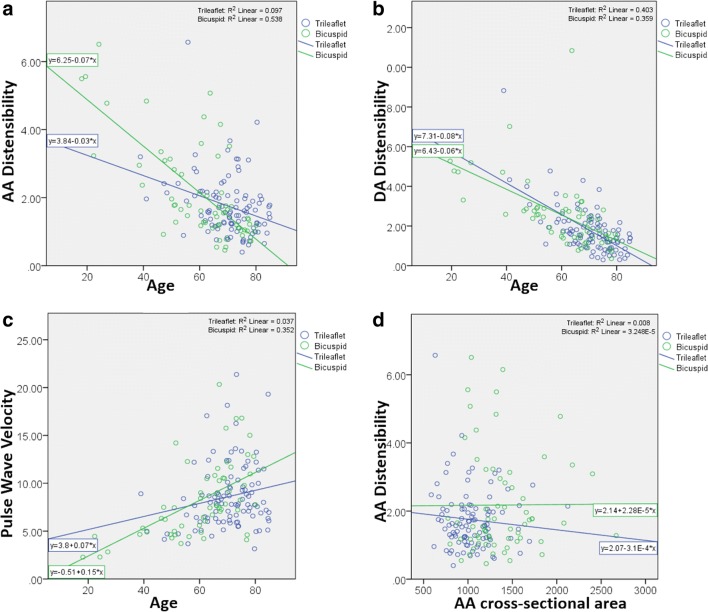
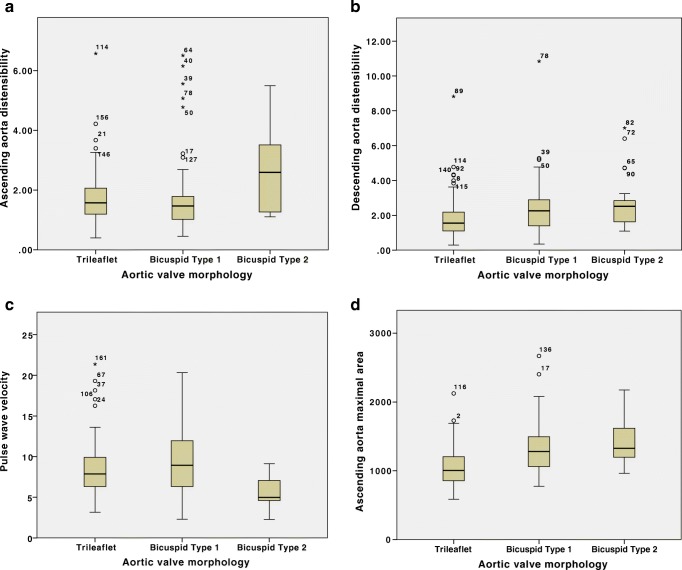
Results: The AA and DA areas were lower in the controls, with no difference in DA distensibility or PWV, but slightly lower AA distensibility than in the patient group. With increasing age, there was a decrease in distensibility and an increase in PWV. After correcting for age, the AA maximum cross-sectional area was higher in bicuspid vs. tricuspid patients (12.97 [11.10, 15.59] vs. 10.06 [8.57, 12.04] cm2, p < 0.001), but there were no significant differences in AA distensibility (p = 0.099), DA distensibility (p = 0.498) or PWV (p = 0.235). Patients with BAV type-II valves demonstrated a significantly higher AA distensibility and lower PWV compared to type-I, despite a trend towards higher AA area.
Conclusions: In patients with significant AS, BAV patients do not have increased aortic stiffness compared to those with TAV despite increased ascending aortic dimensions. Those with type-II BAV have less aortic stiffness despite greater dimensions. These results demonstrate a dissociation between aortic dilatation and stiffness and suggest that altered flow patterns may play a role.
Key points: • Both cellular abnormalities secondary to genetic differences and abnormal flow patterns have been implicated in the pathophysiology of aortic dilatation and increased vascular complications associated with bicuspid aortic valves (BAV). • We demonstrate an increased ascending aortic size in patients with BAV and moderate to severe AS compared to TAV and controls, but no difference in aortic stiffness parameters, therefore suggesting a dissociation between dilatation and stiffness. • Sub-group analysis showed greater aortic size but lower stiffness parameters in those with BAV type-II AS compared to BAV type-I.
Keywords: Aorta, thoracic; Aortic valve stenosis; Aortic valve, bicuspid; Magnetic resonance imaging; Pulse wave velocity.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is Professor Gerry McCann.
Conflict of interest
MAH is the owner of Xinapse Systems software which was used to quantify distensibility and PWV in this study. There are no other competing interests to declare.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was obtained from all subjects before participation.
Ethical approval
The study was approved by the United Kingdom National Research Ethics Service (11/EM/0410).
Study subjects or cohort overlaps
Some study subjects have been previously reported in the main results of the PRIMID-AS study (as mentioned in reference 15 under the “Materials and methods” section of the manuscript). However, the aortic stiffness parameters are novel in this manuscript, as is the comparison of bicuspid and tricuspid sub-groups.
Methodology
• Prospective
• Multi-centre
• Observational study
Figures
Similar articles
-
Influence of Aortic Dilation on the Regional Aortic Stiffness of Bicuspid Aortic Valve Assessed by 4-Dimensional Flow Cardiac Magnetic Resonance: Comparison With Marfan Syndrome and Degenerative Aortic Aneurysm.JACC Cardiovasc Imaging. 2019 Jun;12(6):1020-1029. doi: 10.1016/j.jcmg.2018.03.017. Epub 2018 May 16. JACC Cardiovasc Imaging. 2019. PMID: 29778849
-
Comprehensive assessment of local and regional aortic stiffness in patients with tricuspid or bicuspid aortic valve aortopathy using magnetic resonance imaging.Int J Cardiol. 2021 Mar 1;326:206-212. doi: 10.1016/j.ijcard.2020.11.046. Epub 2020 Nov 28. Int J Cardiol. 2021. PMID: 33259874
-
Patterns of ascending aortic dilatation and predictors of surgical replacement of the aorta: A comparison of bicuspid and tricuspid aortic valve patients over eight years of follow-up.J Mol Cell Cardiol. 2019 Oct;135:31-39. doi: 10.1016/j.yjmcc.2019.07.010. Epub 2019 Jul 23. J Mol Cell Cardiol. 2019. PMID: 31348923 Clinical Trial.
-
Multimodality imaging in bicuspid aortic valve.Prog Cardiovasc Dis. 2020 Jul-Aug;63(4):442-451. doi: 10.1016/j.pcad.2020.06.003. Epub 2020 Jun 9. Prog Cardiovasc Dis. 2020. PMID: 32531300 Review.
-
Functional assessment of thoracic aortic aneurysms - the future of risk prediction?Br Med Bull. 2017 Jan 1;121(1):61-71. doi: 10.1093/bmb/ldw049. Br Med Bull. 2017. PMID: 27989994 Free PMC article. Review.
Cited by
-
The role of 4-dimensional flow in the assessment of bicuspid aortic valve and its valvulo-aortopathies.Br J Radiol. 2022 Oct 1;95(1139):20220123. doi: 10.1259/bjr.20220123. Epub 2022 Aug 3. Br J Radiol. 2022. PMID: 35852109 Free PMC article. Review.
-
Arterial Stiffness in Aortic Stenosis.Arq Bras Cardiol. 2021 Mar;116(3):483-484. doi: 10.36660/abc.20201234. Arq Bras Cardiol. 2021. PMID: 33909778 Free PMC article. English, Portuguese. No abstract available.
-
Aortic wall shear stress in bicuspid aortic valve disease-10-year follow-up.Cardiovasc Diagn Ther. 2023 Feb 28;13(1):38-50. doi: 10.21037/cdt-22-477. Epub 2023 Feb 10. Cardiovasc Diagn Ther. 2023. PMID: 36864959 Free PMC article.
-
Clinical implications of the biomechanics of bicuspid aortic valve and bicuspid aortopathy.Front Cardiovasc Med. 2022 Aug 12;9:922353. doi: 10.3389/fcvm.2022.922353. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36035900 Free PMC article. Review.
-
Resource efficient aortic distensibility calculation by end to end spatiotemporal learning of aortic lumen from multicentre multivendor multidisease CMR images.Sci Rep. 2023 Dec 8;13(1):21794. doi: 10.1038/s41598-023-48986-6. Sci Rep. 2023. PMID: 38066222 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
