

Weight restoration in atypical anorexia nervosa: A clinical conundrum
- PMID: 30488483
- PMCID: PMC6295247
- DOI: 10.1002/eat.22953
Weight restoration in atypical anorexia nervosa: A clinical conundrum
Abstract
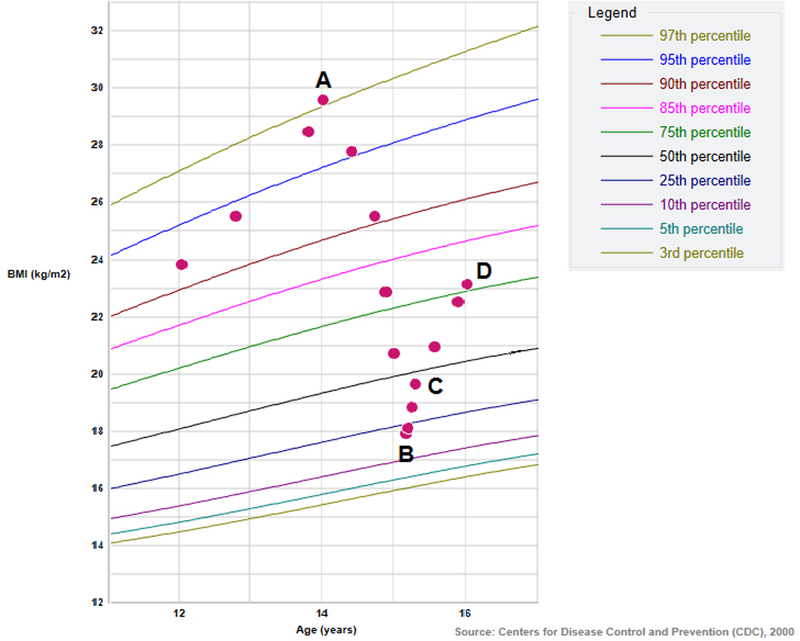
The determination of the treatment goal weight for adolescents with a restrictive eating disorder (ED) and a prior history of obesity, such as in atypical anorexia nervosa (AAN), represents an ongoing challenge for clinicians. This determination is particularly complex given competing interests of physical recovery from significant weight loss, mental recovery from ED psychopathology, and the medical comorbidities associated with obesity. We report the case of a 15-year old female with a history of obesity and irregular periods who presented with significant weight loss and absence of menses for 3 months. She was hospitalized for severe malnutrition and bradycardia, initiated family based treatment, and regained periods. However, her vital sign instability and eating disorder cognitions did not resolve until she reached a weight at which point her periods again ceased due to polycystic ovary syndrome. This case highlights the need for regular monitoring during weight recovery and the clinical challenge of determining the treatment goal weight in adolescents with EDs and prior obesity.
Keywords: amenorrhea; atypical anorexia nervosa; eating disorders; obesity; overweight; polycystic ovary syndrome.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
Figures
Similar articles
-
Adolescents with anorexia nervosa or atypical anorexia nervosa with premorbid overweight/obesity: What should we do about their weight loss?J Child Adolesc Psychiatr Nurs. 2023 Feb;36(1):55-58. doi: 10.1111/jcap.12394. Epub 2022 Sep 19. J Child Adolesc Psychiatr Nurs. 2023. PMID: 36121167
-
Associations between presenting weight and premorbid weight and the medical sequelae in hospitalized youth with anorexia nervosa or atypical anorexia nervosa.J Pediatr Nurs. 2024 Jul-Aug;77:125-130. doi: 10.1016/j.pedn.2024.03.013. Epub 2024 Mar 21. J Pediatr Nurs. 2024. PMID: 38518688
-
Predictors of Complications in Anorexia Nervosa and Atypical Anorexia Nervosa: Degree of Underweight or Extent and Recency of Weight Loss?J Adolesc Health. 2018 Dec;63(6):717-723. doi: 10.1016/j.jadohealth.2018.08.019. J Adolesc Health. 2018. PMID: 30454732
-
Medical instability in typical and atypical adolescent anorexia nervosa: a systematic review and meta-analysis.J Eat Disord. 2023 Apr 6;11(1):58. doi: 10.1186/s40337-023-00779-y. J Eat Disord. 2023. PMID: 37024943 Free PMC article. Review.
-
Atypical Anorexia in Youth: Cautiously Bridging the Treatment Gap.Children (Basel). 2022 Jun 5;9(6):837. doi: 10.3390/children9060837. Children (Basel). 2022. PMID: 35740774 Free PMC article. Review.
Cited by
-
Comparison of clinical presentation and treatment response among youth with atypical anorexia nervosa and anorexia nervosa.PLoS One. 2025 Mar 4;20(3):e0316572. doi: 10.1371/journal.pone.0316572. eCollection 2025. PLoS One. 2025. PMID: 40036217 Free PMC article.
-
TeenGrowth: Individualized Estimations of Weight-Related Risk and Recovery Metrics for Young People With Eating Disorders.Int J Eat Disord. 2025 Apr;58(4):658-668. doi: 10.1002/eat.24372. Epub 2025 Jan 6. Int J Eat Disord. 2025. PMID: 39760235
-
Weighing in: Clinician and Patient Perspectives on Discussions of Expected Body Weights in Eating Disorder Treatment.Int J Eat Disord. 2025 Jul 7:10.1002/eat.24501. doi: 10.1002/eat.24501. Online ahead of print. Int J Eat Disord. 2025. PMID: 40621704
-
What does weight have to do with Atypical AN? A commentary on weight outcomes for adolescents with atypical anorexia nervosa in family-based treatment.J Can Acad Child Adolesc Psychiatry. 2023 Aug;32(3):172-176. Epub 2023 Aug 1. J Can Acad Child Adolesc Psychiatry. 2023. PMID: 37534117 Free PMC article.
-
Estimating Treatment Goal Weights in Adolescents With Anorexia Nervosa and Atypical Anorexia Nervosa: Comparison of the Median BMI and Historical BMI Percentile.Int J Eat Disord. 2024 Dec;57(12):2491-2496. doi: 10.1002/eat.24298. Epub 2024 Sep 26. Int J Eat Disord. 2024. PMID: 39324372 Free PMC article.
References
-
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th Ed. ed.). Arlington, VA: American Psychiatric Publishing.
-
- Bibbins-Domingo K, Coxson P, Pletcher MJ, Lightwood J, & Goldman L (2007). Adolescent overweight and future adult coronary heart disease. The New England Journal of Medicine, 357(23), 2371–2379. 10.1056/NEJMsa073166 - DOI - PubMed
-
- Centers for Disease Control. (2000). Growth charts Retrieved from http://www.cdc.gov/growthcharts/
-
- Golden NH, Katzman DK, Sawyer SM, Ornstein RM, Rome ES, Garber AK, … Kreipe RE. (2015). Update on the medical management of eating disorders in adolescents. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 56(4), 370–375. 10.1016/j.jadohealth.2014.11.020 - DOI - PubMed
-
- Hughes EK, Le Grange D, Court A, & Sawyer SM (2017). A case series of family-based treatment for adolescents with atypical anorexia nervosa. The International Journal of Eating Disorders, 50(4), 424–432. 10.1002/eat.22662 - DOI - PubMed
