

Integrated outpatient palliative care for patients with advanced cancer: A systematic review and meta-analysis
- PMID: 30488781
- PMCID: PMC7069657
- DOI: 10.1177/0269216318812633
Integrated outpatient palliative care for patients with advanced cancer: A systematic review and meta-analysis
Abstract
Background:: Despite increasing emphasis on integration of palliative care with disease-directed care for advanced cancer, the nature of this integration and its effects on patient and caregiver outcomes are not well-understood.
Aim:: We evaluated the effects of integrated outpatient palliative and oncology care for advanced cancer on patient and caregiver outcomes.
Design:: Following a standard protocol (PROSPERO: CRD42017057541), investigators independently screened reports to identify randomized controlled trials or quasi-experimental studies that evaluated the effect of integrated outpatient palliative and oncology care interventions on quality of life, survival, and healthcare utilization among adults with advanced cancer. Data were synthesized using random-effects meta-analyses, supplemented with qualitative methods when necessary.
Data sources:: English-language peer-reviewed publications in PubMed, CINAHL, and Cochrane Central through November 2016. We subsequently updated our PubMed search through July 2018.
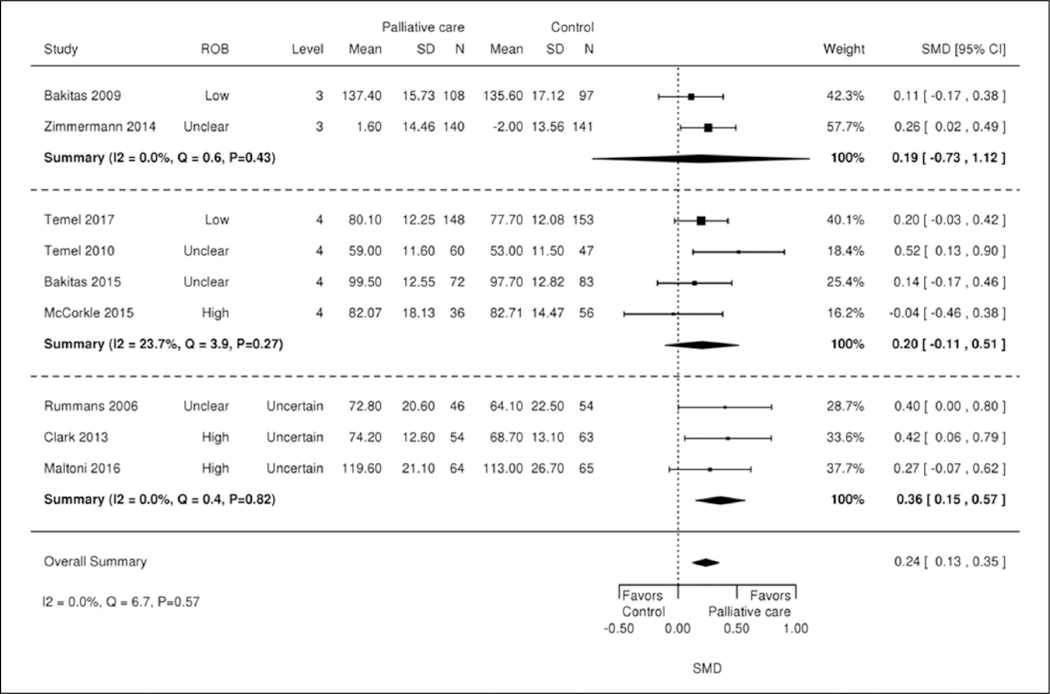
Results:: Eight randomized-controlled and two cluster-randomized trials were included. Most patients had multiple advanced cancers, with median time from diagnosis or recurrence to enrollment ranging from 8 to 12 weeks. All interventions included a multidisciplinary team, were classified as “moderately integrated,” and addressed physical and psychological symptoms. In a meta-analysis, short-term quality of life improved, symptom burden improved, and all-cause mortality decreased. Qualitative analyses revealed no association between integration elements, palliative care intervention elements, and intervention impact. Utilization and caregiver outcomes were often not reported.
Conclusions:: Moderately integrated palliative and oncology outpatient interventions had positive effects on short-term quality of life, symptom burden, and survival. Evidence for effects on healthcare utilization and caregiver outcomes remains sparse.
Keywords: Meta-analysis; palliative care; palliative medicine; quality of life; survival.
Conflict of interest statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Comment in
-
Reading past the p < 0.05's: The secondary messages of systematic reviews and meta-analyses in palliative care.Palliat Med. 2019 Feb;33(2):121-122. doi: 10.1177/0269216318821054. Palliat Med. 2019. PMID: 30799732 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin 2017; 67(3): 177–193. - PubMed
-
- Center to Advance Palliative Care. Definition of palliative care, https://www.capc.org/about/palliative-care/ (accessed 28 July 2017).
-
- Institute of Medicine. Delivering high-quality cancer care: charting a new course for a system in crisis. Washington, DC: National Academies Press, 2013. - PubMed
-
- American Board of Internal Medicine. Hospice & Palliative Medicine Policies, http://www.abim.org/certification/policies/internal-medicine-subspecialt... (accessed 14 July 2017).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
