

Partial Stapled Hemorrhoidopexy Versus Circumferential Stapled Hemorrhoidopexy for Grade III to IV Prolapsing Hemorrhoids: A Randomized, Noninferiority Trial
- PMID: 30489326
- PMCID: PMC6365260
- DOI: 10.1097/DCR.0000000000001261
Partial Stapled Hemorrhoidopexy Versus Circumferential Stapled Hemorrhoidopexy for Grade III to IV Prolapsing Hemorrhoids: A Randomized, Noninferiority Trial
Abstract
Background: Long-term outcomes and efficacy of partial stapled hemorrhoidopexy are not known.
Objective: The purpose of this study was to compare the long-term clinical efficacy and safety of partial stapled hemorrhoidopexy with circumferential stapled hemorrhoidopexy.
Design: This was a parallel group, randomized, noninferiority clinical trial.
Settings: The study was conducted at a single academic center.
Patients: Patients with grade III/IV hemorrhoids between August 2011 and November 2013 were included.
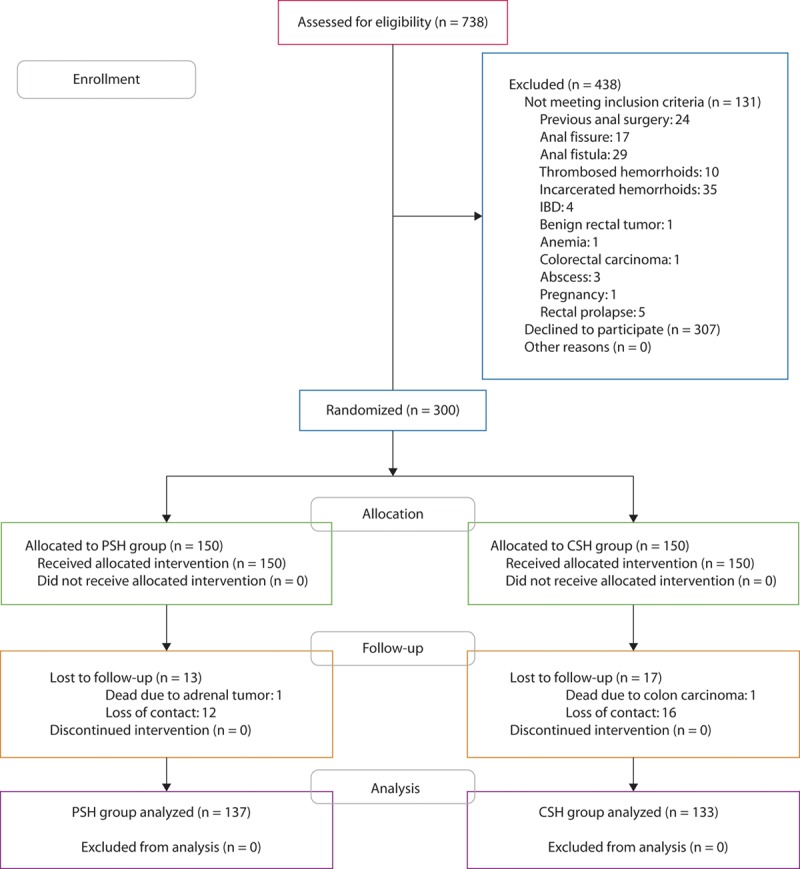
Interventions: Three hundred patients were randomly assigned to undergo either partial stapled hemorrhoidopexy (group 1, n = 150) or circumferential stapled hemorrhoidopexy (group 2, n = 150).
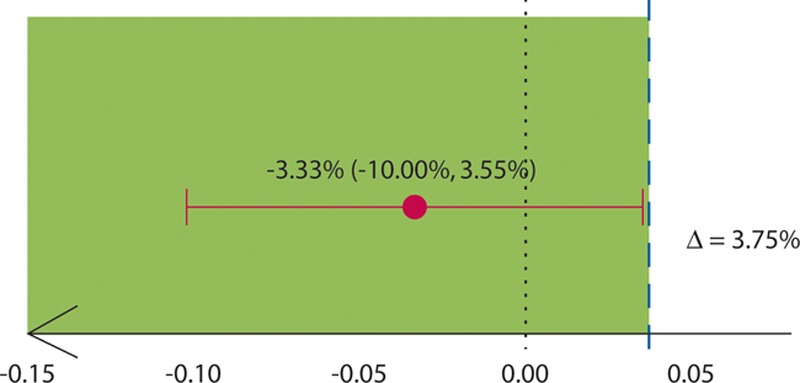
Main outcome measures: The primary outcome was the rate of recurrent prolapse at a median follow-up period of 5 years with a predefined noninferiority margin of 3.75%. Secondary outcomes included incidence and severity of postoperative pain, fecal urgency, anal continence, and the frequency of specific complications, including anorectal stenosis and rectovaginal fistula.
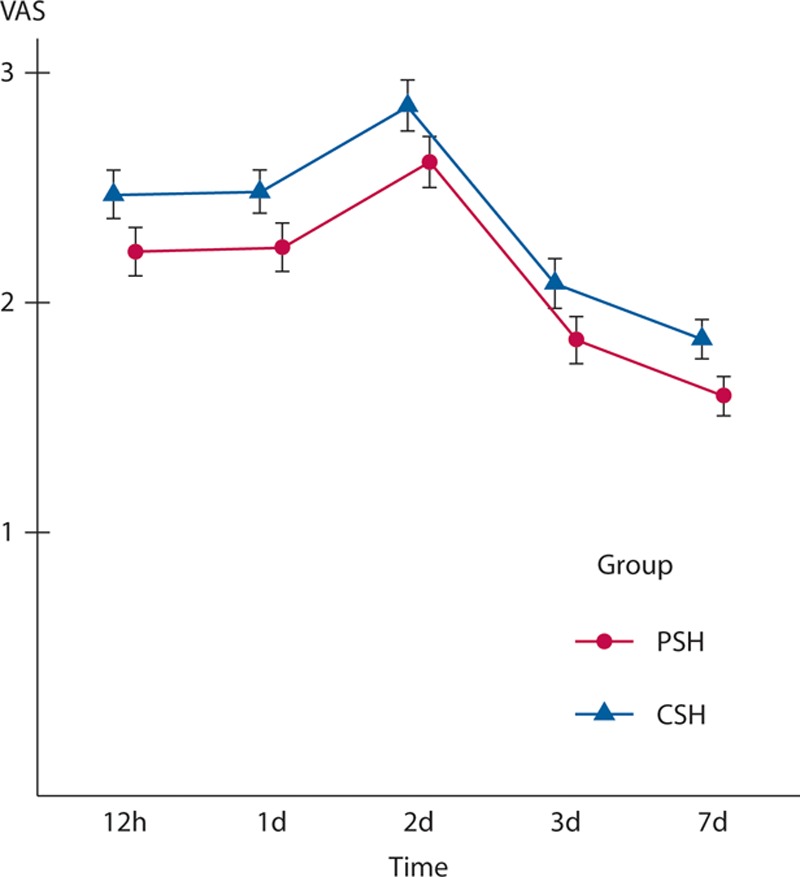
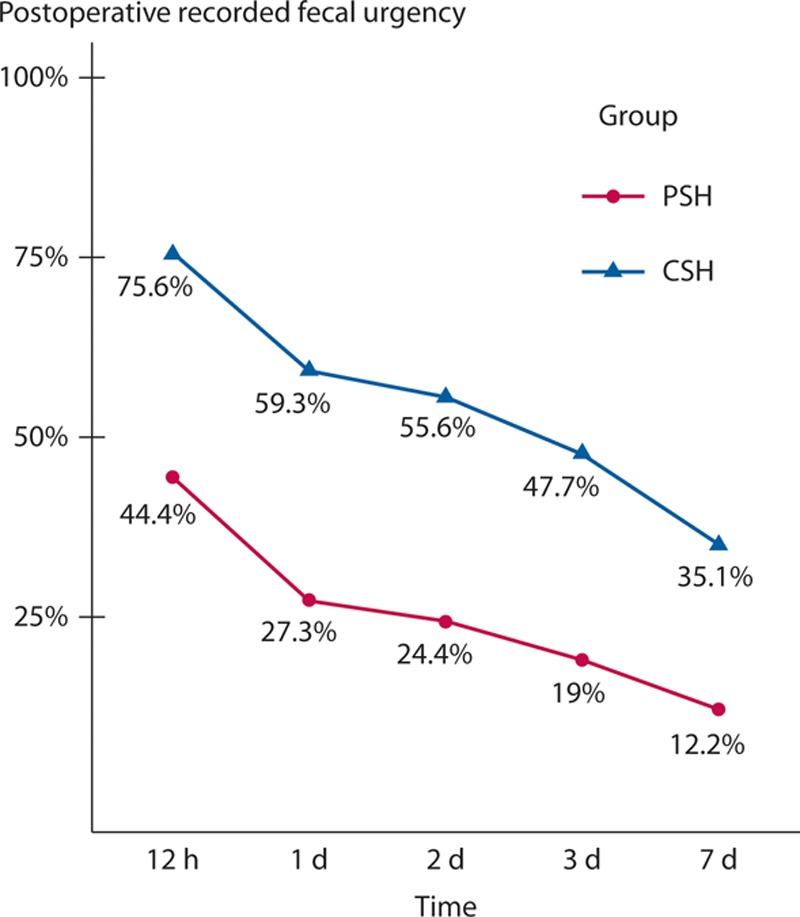
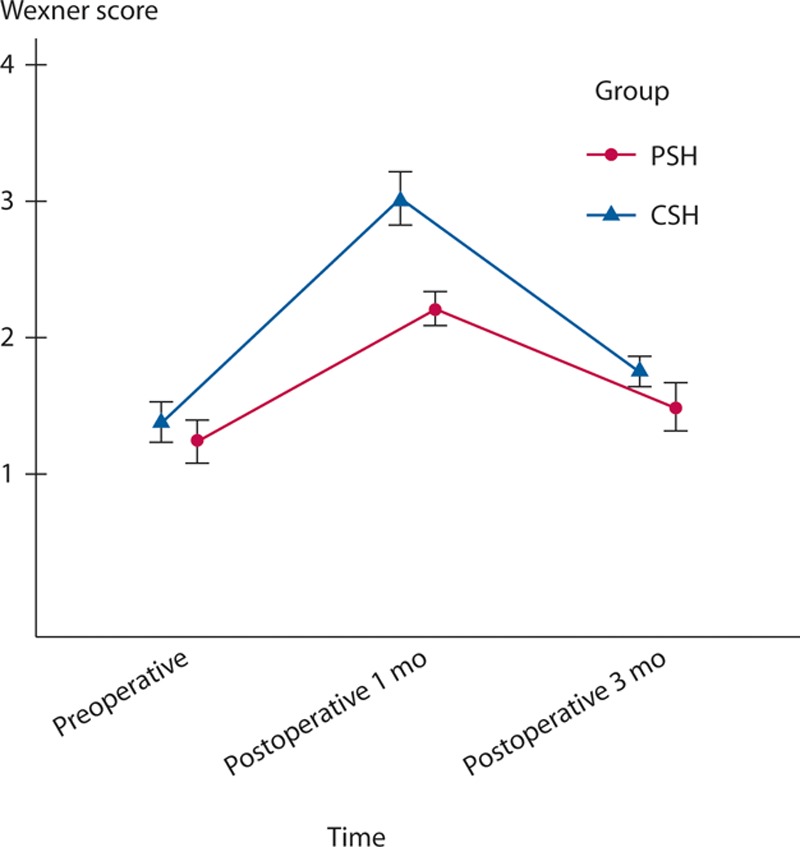
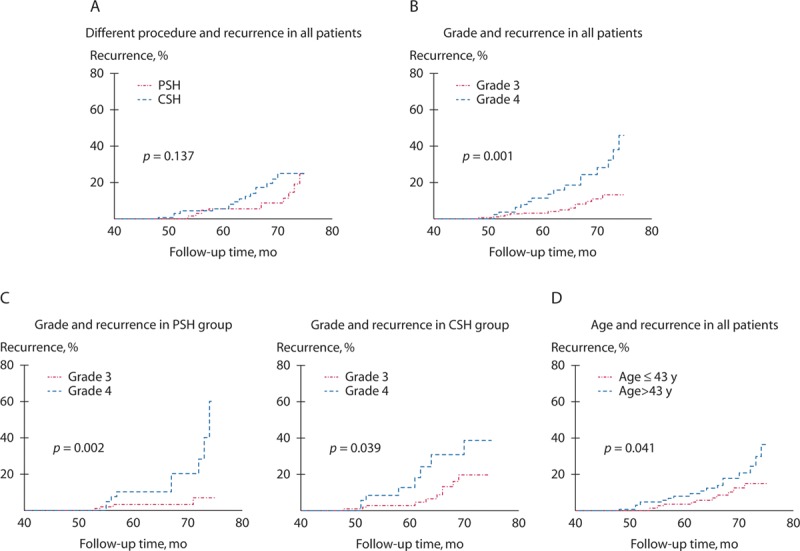
Results: The visual analog scores in group 1 were less than those in group 2 (p < 0.001). Fewer patients in group 1 experienced postoperative urgency compared with those in group 2 (p = 0.001). Anal continence significantly worsened after both procedures, but the difference between preoperative and postoperative continence scores was higher for group 2 than for group 1. Postoperative rectal stenosis did not develop in patients in group 1, although it occurred in 8 patients (5%) in group 2 (p = 0.004). The 5-year cumulative recurrence rate between group 1 (9% (95% CI, 4%-13%)) and group 2 (12% (95% CI, 7%-17%)) did not differ significantly (p = 0.137), and the difference was within the noninferiority margin (absolute difference, -3.33% (95% CI, -10.00% to 3.55%)).
Limitations: The study was limited because it was a single-center trial.
Conclusions: Partial stapled hemorrhoidopexy is noninferior to circumferential stapled hemorrhoidopexy for patients with grade III to IV hemorrhoids at a median follow-up period of 5 years. However, partial stapled hemorrhoidopexy was associated with reduced postoperative pain and urgency, better postoperative anal continence, and minimal risk of rectal stenosis. See Video Abstract at http://links.lww.com/DCR/A790.Trial registration (chictr.org) identifier is chiCTR-trc-11001506.
Figures
Similar articles
-
Partial stapled hemorrhoidopexy versus circular stapled hemorrhoidopexy for grade III-IV prolapsing hemorrhoids: a two-year prospective controlled study.Tech Coloproctol. 2012 Oct;16(5):337-43. doi: 10.1007/s10151-012-0815-8. Epub 2012 Mar 9. Tech Coloproctol. 2012. PMID: 22402919 Clinical Trial.
-
Stapled hemorrhoidopexy versus milligan-morgan hemorrhoidectomy: a prospective, randomized, multicenter trial with 2-year postoperative follow up.Ann Surg. 2005 Jul;242(1):29-35. doi: 10.1097/01.sla.0000169570.64579.31. Ann Surg. 2005. PMID: 15973098 Free PMC article. Clinical Trial.
-
Long-term outcomes after circular stapled hemorrhoidopexy versus Ferguson hemorrhoidectomy.Tech Coloproctol. 2015 Oct;19(10):653-8. doi: 10.1007/s10151-015-1366-6. Epub 2015 Sep 10. Tech Coloproctol. 2015. PMID: 26359179
-
Stapled hemorrhoidopexy vs. diathermy excision for fourth-degree hemorrhoids: a randomized, clinical trial and review of the literature.Dis Colon Rectum. 2005 Apr;48(4):809-15. doi: 10.1007/s10350-004-0861-z. Dis Colon Rectum. 2005. PMID: 15785901 Review.
-
Transanal hemorrhoidal dearterialization (THD) versus stapled hemorrhoidopexy (SH) in treatment of internal hemorrhoids: a systematic review and meta-analysis of randomized clinical trials.Int J Colorectal Dis. 2019 Jan;34(1):1-11. doi: 10.1007/s00384-018-3187-3. Epub 2018 Nov 12. Int J Colorectal Dis. 2019. PMID: 30421308
Cited by
-
A comparative study on efficacy and safety of modified partial stapled hemorrhoidopexy versus conventional hemorrhoidectomy: a prospective randomized controlled trial.Ann Coloproctol. 2025 Apr;41(2):145-153. doi: 10.3393/ac.2024.00535.0076. Epub 2025 Apr 28. Ann Coloproctol. 2025. PMID: 40313128 Free PMC article.
-
Correlation Between Poor Defecation Habits and Postoperative Hemorrhoid Recurrence.Front Surg. 2022 Jun 17;9:930215. doi: 10.3389/fsurg.2022.930215. eCollection 2022. Front Surg. 2022. PMID: 35784912 Free PMC article.
-
Electroacupuncture at Baliao point alleviates post-operative pain and anal distension after procedure for prolapse and hemorrhoids (stapled hemorrhoidopexy): a prospective randomized clinical trial.Int J Colorectal Dis. 2023 Apr 19;38(1):104. doi: 10.1007/s00384-023-04403-y. Int J Colorectal Dis. 2023. PMID: 37074488 Free PMC article. Clinical Trial.
-
The comparison of an accessible C-shaped partial stapled hemorrhoidopexy (C-PSH) versus circular stapled hemorrhoidopexy (CSH) in patients with grade IV hemorrhoids: a retrospective cohort study.BMC Gastroenterol. 2023 Dec 16;23(1):443. doi: 10.1186/s12876-023-03062-1. BMC Gastroenterol. 2023. PMID: 38104065 Free PMC article.
-
The efficiency and safety of modified tissue-selecting therapy stapler combined with complete anal canal epithelial preservation operation in circumferential mixed hemorrhoids: a randomized controlled trial.Langenbecks Arch Surg. 2023 Aug 24;408(1):332. doi: 10.1007/s00423-023-03081-2. Langenbecks Arch Surg. 2023. PMID: 37620667 Clinical Trial.
References
-
- Longo A. Treatment of hemorrhoidal disease by reduction of mucosa and hemorrhoidal prolapse with a circular suturing device: a new procedure. In: Proceedings of the 6th World Congress of Endoscopic Surgery. 1998:Bologna, Italy: Monduzzi Editore; 777–784..
-
- Shao WJ, Li GC, Zhang ZH, Yang BL, Sun GD, Chen YQ. Systematic review and meta-analysis of randomized controlled trials comparing stapled haemorrhoidopexy with conventional haemorrhoidectomy. Br J Surg. 2008;95:147–160.. - PubMed
-
- Garg P, Sidhu G, Nair S, et al. The fate and significance of retained staples after stapled haemorrhoidopexy. Colorectal Dis. 2011;13:572–575.. - PubMed
-
- Naldini G. Serious unconventional complications of surgery with stapler for haemorrhoidal prolapse and obstructed defaecation because of rectocoele and rectal intussusception. Colorectal Dis. 2011;13:323–327.. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
