

Persistent inflammation and anemia among critically ill septic patients
- PMID: 30489504
- PMCID: PMC6410351
- DOI: 10.1097/TA.0000000000002147
Persistent inflammation and anemia among critically ill septic patients
Abstract
Background: Associations among inflammatory cytokines, erythropoietin (EPO), and anemia in critically ill septic patients remain unclear. This study tested the hypothesis that elevated inflammatory cytokines and decreased EPO would be associated with iron-restricted anemia while accounting for operative blood loss, phlebotomy blood loss, and red blood cell (RBC) transfusion volume.
Methods: Prospective observational cohort study of 42 critically ill septic patients was conducted. Hemoglobin (Hb) at sepsis onset and hospital discharge were used to calculate ΔHb. Operative blood loss, phlebotomy blood loss, and RBC transfusion volume were used to calculate adjusted ΔHb (AdjΔHb) assuming that 300 mL RBC is equal to 1 g/dL Hb. Patients with AdjΔHb of greater than 0 (positive AdjΔHb, n = 18) were compared with patients with AdjΔHb of less than or equal to 0 (negative AdjΔHb, n = 24).
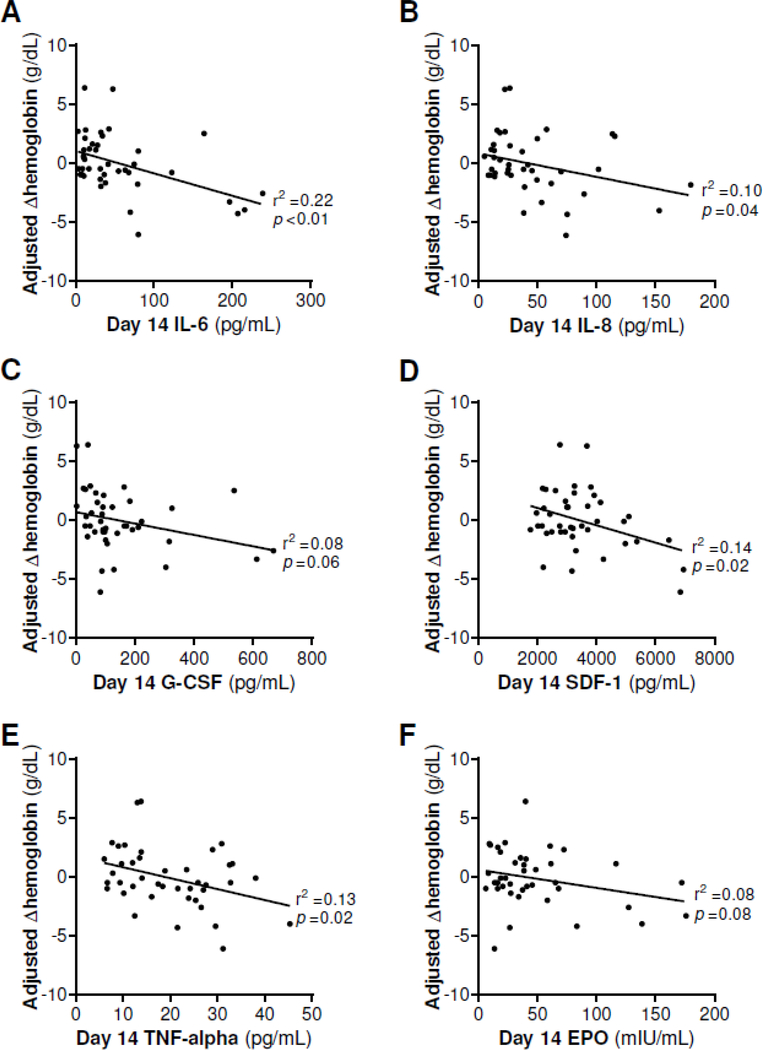
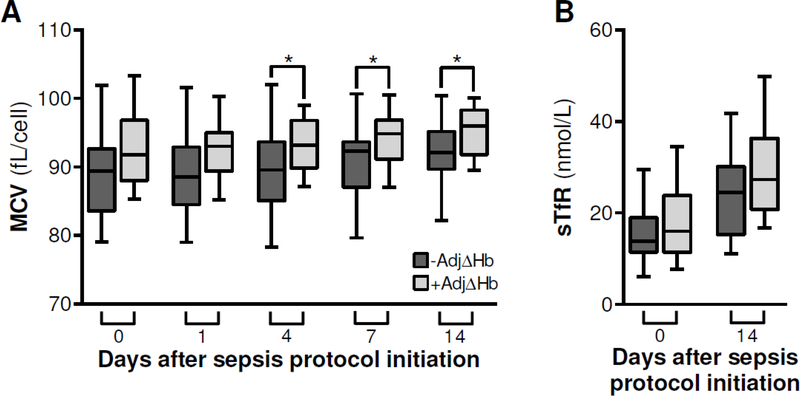
Results: Plasma tumor necrosis factor α, granulocyte colony-stimulating factor, interleukin (IL)-6, IL-8, EPO, erythrocyte mean corpuscular volume, and serum transferrin receptor were measured on days 0, 1, 4, 7, and 14. Patients with negative AdjΔHb had significantly higher day 14 levels of IL-6 (37.4 vs. 15.2 pg/mL, p < 0.05), IL-8 (39.1 vs. 18.2 pg/mL, p = 0.01), and granulocyte colony-stimulating factor (101.3 vs. 60.5 pg/mL, p = 0.01), but not EPO. On linear regression analysis, lower AdjΔHb was associated with higher day 14 levels of IL-6 (r = 0.22, p < 0.01), IL-8 (r = 0.10, p = 0.04), stromal cell-derived factor 1 (r = 0.14, p = 0.02), and tumor necrosis factor α (r = 0.13, p = 0.02), but not EPO. Patients with negative AdjΔHb had significantly lower mean corpuscular volume on days 4 (89.6 vs. 93.2 fL/cell, p = 0.04), 7 (92.3 vs. 94.9 fL/cell, p = 0.04), and 14 (92.1 vs. 96.0 fL/cell, p = 0.03) but similar serum transferrin receptor levels.
Conclusion: Persistent elevation of inflammatory cytokines was associated with iron-restricted anemia among critically ill septic patients, occurring in the absence of systemic iron deficiency, independent of endogenous EPO.
Level of evidence: Prognostic study, level II.
Figures

Similar articles
-
Serum Soluble-Fas, Inflammation, and Anemia in Acute Kidney Injury.Artif Organs. 2018 Sep;42(9):E283-E289. doi: 10.1111/aor.12019. Epub 2013 Apr 9. Artif Organs. 2018. PMID: 23566289
-
The effects of beta blockade and clonidine on persistent injury-associated anemia.J Surg Res. 2018 Oct;230:175-180. doi: 10.1016/j.jss.2018.06.001. Epub 2018 Jun 28. J Surg Res. 2018. PMID: 29960715 Free PMC article.
-
The effect of red blood cell transfusion on iron metabolism in critically ill patients.Transfusion. 2019 Apr;59(4):1196-1201. doi: 10.1111/trf.15127. Epub 2018 Dec 31. Transfusion. 2019. PMID: 30597563
-
The role of erythropoietin therapy in the critically ill.Transfus Med Rev. 2006 Jan;20(1):27-33. doi: 10.1016/j.tmrv.2005.08.002. Transfus Med Rev. 2006. PMID: 16373185 Review.
-
Anemia in the critically ill.Crit Care Clin. 2004 Apr;20(2):159-78. doi: 10.1016/j.ccc.2004.01.002. Crit Care Clin. 2004. PMID: 15135458 Review.
Cited by
-
Development and performance evaluation of a clinical prediction model for sepsis risk in burn patients.Medicine (Baltimore). 2024 Nov 29;103(48):e40709. doi: 10.1097/MD.0000000000040709. Medicine (Baltimore). 2024. PMID: 39612449 Free PMC article.
-
Multiple organ failure: What you need to know.J Trauma Acute Care Surg. 2024 Dec 1;97(6):831-838. doi: 10.1097/TA.0000000000004419. Epub 2024 Sep 3. J Trauma Acute Care Surg. 2024. PMID: 39225733 Review.
-
Effects of Antithrombin on Persistent Inflammation, Immunosuppression, and Catabolism Syndrome among Patients with Sepsis-Induced Disseminated Intravascular Coagulation.J Clin Med. 2023 Jun 2;12(11):3822. doi: 10.3390/jcm12113822. J Clin Med. 2023. PMID: 37298017 Free PMC article.
-
Chronic Critical Illness in Patients With Sepsis is Associated With Persistent Anemia, Inflammation, and Impaired Functional Outcomes.Am Surg. 2023 Jun;89(6):2563-2571. doi: 10.1177/00031348221104252. Epub 2022 May 20. Am Surg. 2023. PMID: 35593749 Free PMC article.
-
Mortality and morbidity of low-grade red blood cell transfusions in septic patients: a propensity score-matched observational study of a liberal transfusion strategy.Ann Intensive Care. 2020 Aug 8;10(1):111. doi: 10.1186/s13613-020-00727-y. Ann Intensive Care. 2020. PMID: 32770427 Free PMC article.
References
-
- Rodriguez RM, Corwin HL, Gettinger A, Corwin MJ, Gubler D, Pearl RG. Nutritional deficiencies and blunted erythropoietin response as causes of the anemia of critical illness. J Crit Care. 2001;16(1):36–41. - PubMed
-
- Vincent JL, Baron JF, Reinhart K, Gattinoni L, Thijs L, Webb A, Meier-Hellmann A, Nollet G, Peres-Bota D, Investigators ABC. Anemia and blood transfusion in critically ill patients. JAMA. 2002;288(12):1499–507. - PubMed
-
- Corwin HL, Parsonnet KC, Gettinger A. RBC transfusion in the ICU. Is there a reason? Chest. 1995;108(3):767–71. - PubMed
-
- Rogiers P, Zhang H, Leeman M, Nagler J, Neels H, Melot C, Vincent JL. Erythropoietin response is blunted in critically ill patients. Intens Care Med. 1997;23(2):159–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
