

Survival, local control, and health-related quality of life in patients with oligometastatic and polymetastatic spinal tumors: A multicenter, international study
- PMID: 30489634
- PMCID: PMC8020734
- DOI: 10.1002/cncr.31870
Survival, local control, and health-related quality of life in patients with oligometastatic and polymetastatic spinal tumors: A multicenter, international study
Abstract
Background: The treatment of oligometastatic (≤5 metastases) spinal disease has trended toward ablative therapies, yet to the authors' knowledge little is known regarding the prognosis of patients presenting with oligometastatic spinal disease and the value of this approach. The objective of the current study was to compare the survival and clinical outcomes of patients with cancer with oligometastatic spinal disease with those of patients with polymetastatic (>5 metastases) disease.
Methods: The current study was an international, multicenter, prospective study. Patients who were admitted to a participating spine center with a diagnosis of spinal metastases and who underwent surgical intervention and/or radiotherapy between August 2013 and May 2017 were included. Data collected included demographics, overall survival, local control, and treatment information including surgical, radiotherapy, and systemic therapy details. Health-related quality of life (HRQOL) measures included the EuroQOL 5 dimensions 3-level questionnaire (EQ-5D-3L), the 36-Item Short Form Health Survey (SF-36v2), and the Spine Oncology Study Group Outcomes Questionnaire (SOSGOQ).
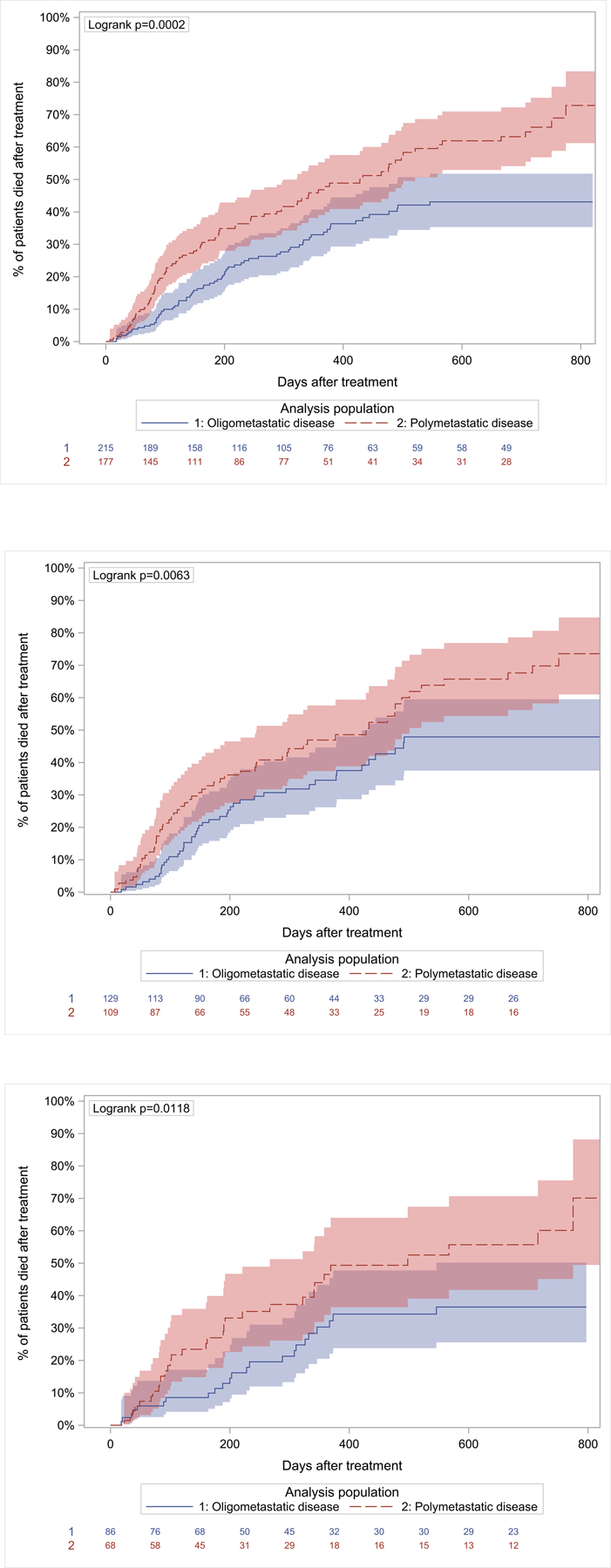
Results: Of the 393 patients included in the current study, 215 presented with oligometastatic disease and 178 presented with polymetastatic disease. A significant survival advantage of 90.1% versus 77.3% at 3 months and 77.0% versus 65.1% at 6 months from the time of treatment was found for patients presenting with oligometastatic disease compared with those with polymetastatic disease. It is important to note that both groups experienced significant improvements in multiple HRQOL measures at 6 months after treatment, with no differences in these outcome measures noted between the 2 groups.
Conclusions: The treatment of oligometastatic disease appears to offer a significant survival advantage compared with polymetastatic disease, regardless of treatment choice. HRQOL measures were found to improve in both groups, demonstrating a palliative benefit for all treated patients.
Keywords: health-related quality of life (HRQOL); oligometastases; polymetastases; spine; survival; tumor.
© 2018 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Ori Barzilai has received fellowship support to his institution from Globus for work performed outside of the current study. Anne L. Versteeg has received consulting and travel accommodations from AOSpine International for work performed outside of the current study. Arjun Sahgal has acted as a paid advisor for AbbVie; has taken part in past educational seminars with Elekta AB, Accuray Inc, Varian Medical Systems, and Brainlab; has received a research grant from Elekta AB; has received travel accommodations and expenses from Elekta AB, Varian Medical Systems, and Brainlab; and is a member of the Elekta MR Linac Research Consortium for work performed outside of the current study. Laurence D. Rhines has educational commitments with Stryker for work performed outside of the current study. Mark H. Bilsky has acted as a member of the Speaker’s Bureau for Varian Medical Systems and Brainlab, has received royalties from DePuy Synthes, and has received royalties/fellowship support from Globus Spine for work performed outside of the current study. Daniel M. Sciubba has acted as a paid consultant for Medtronic, DePuy Synthes, Stryker, NuVasive, K2M, Baxter, and Misonix for work performed outside of the current study. Chetan Bettegowda has acted as a paid consultant for DePuy Synthes for work performed outside of the current study. Yoshiya Yamada has acted as a member of the Speakers’ Bureau for Varian Medical Systems, Brainlab, Vision RT, and the Institute for Medical Education for work performed as part of the current study and has acted as a member of the Medical Advisory Board for the Chordoma Foundation for work performed outside of the current study. Paul M. Arnold has received travel accommodations and expenses from AOSpine North America; has intellectual property rights and interests, equity, and a position of responsibility as part of Evoke Medical; has equity from Z-Plasty; has received consulting fees from Stryker Orthopaedics, Ulrich, SpineGuard, In Vivo Therapeutics, and In Vivo; and has received consulting fees, travel accommodations, and expenses from Stryker Spine, Spine Wave, and Medtronic for work performed outside of the current study. Ziya L. Gokaslan has received research support from AOSpine North America and has stock ownership in Spinal Kinetics for work performed outside of the current study. Charles G. Fisher has received consulting and royalty fees from Medtronic, has received research grants from the Orthopedic Research and Education Foundation, and has received fellowship support paid to his institution from AOSpine and Medtronic for work performed outside of the current study. Ilya Laufer has received personal fees from Globus, Medtronic, DePuy Synthes, Spine Wave, and Brainlab for work performed outside of the current study.
Figures


References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017;67:7–30. - PubMed
-
- Sinson GP, Zager EL. Metastases and spinal cord compression. N Engl J Med 1992;327:1953–1954; author reply 1954–1955. - PubMed
-
- Wong DA, Fornasier VL, MacNab I. Spinal metastases: the obvious, the occult, and the impostors. Spine (Phila Pa 1976). 1990;15:1–4. - PubMed
-
- Tomita K, Kawahara N, Kobayashi T, Yoshida A, Murakami H, Akamaru T. Surgical strategy for spinal metastases. Spine (Phila Pa 1976). 2001;6:298–306. - PubMed
-
- Tokuhashi Y, Matsuzaki H, Oda H, Oshima M, Ryu J. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine (Phila Pa 1976). 2005;30:2186–2191. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
