

Activation of RANK/RANKL/OPG Pathway Is Involved in the Pathophysiology of Fibrous Dysplasia and Associated With Disease Burden
- PMID: 30496606
- PMCID: PMC6983320
- DOI: 10.1002/jbmr.3602
Activation of RANK/RANKL/OPG Pathway Is Involved in the Pathophysiology of Fibrous Dysplasia and Associated With Disease Burden
Abstract
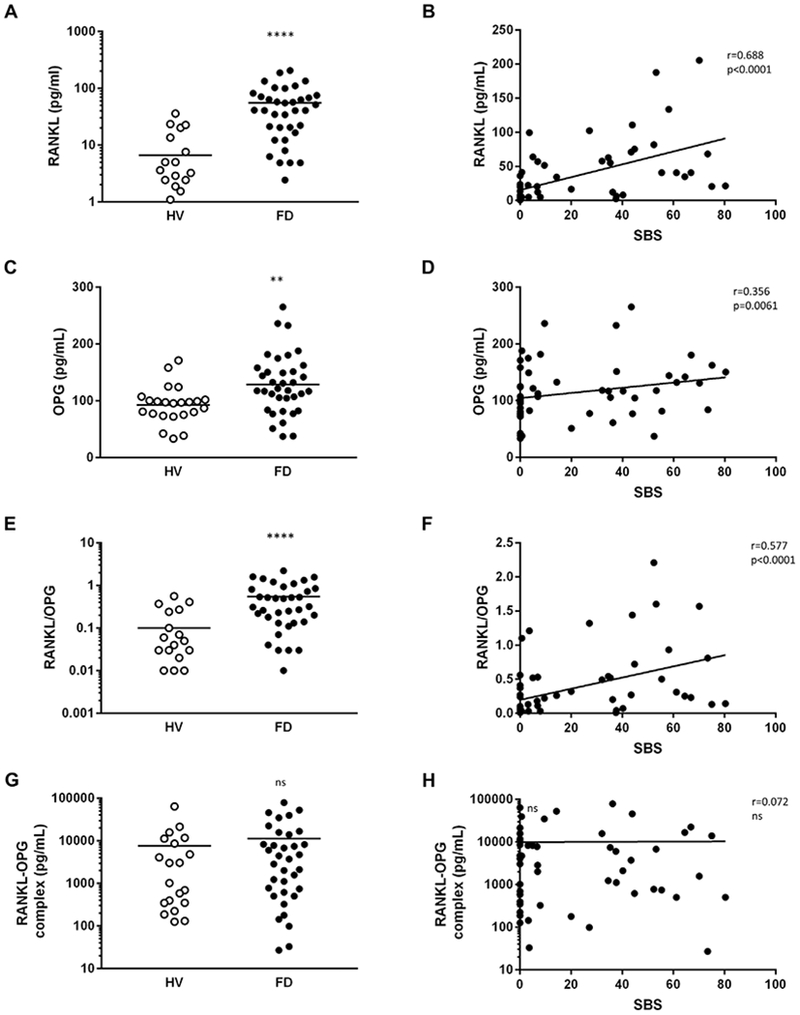
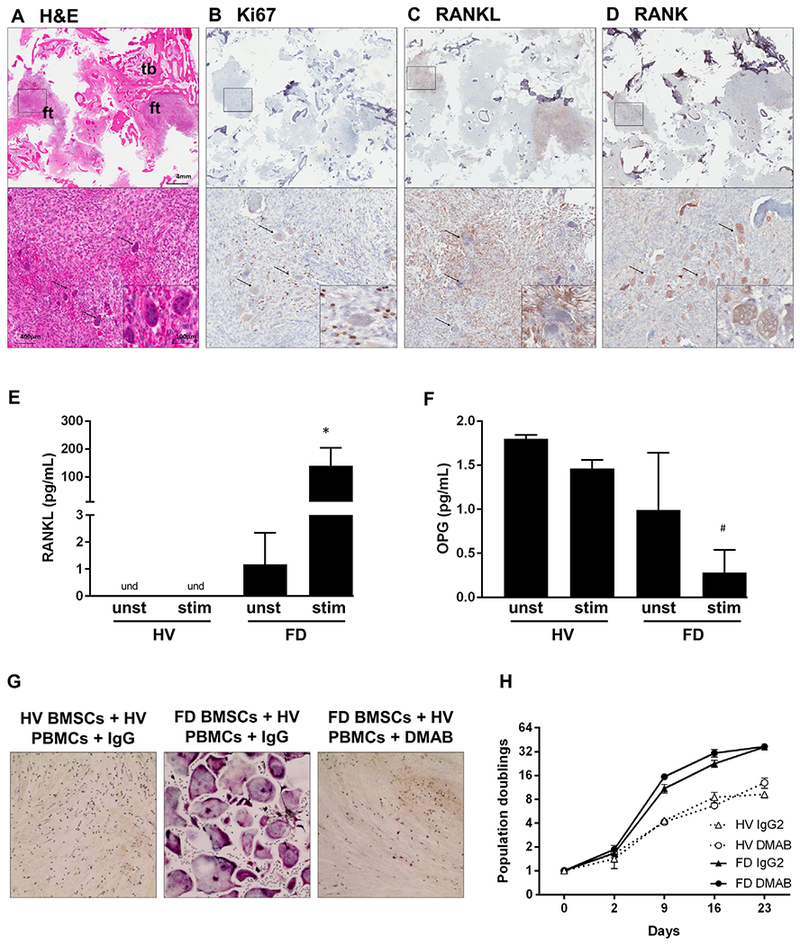
Fibrous dysplasia of bone (FD) is a mosaic disease caused by mutations in GNAS. Constitutive activation of the α-subunit of the Gs stimulatory protein (Gαs) leads to dysregulated proliferation of bone marrow stromal cells (BMSCs), generating expansile lesions of fibrotic tissue and abnormal bone. Local bone remodeling regulation by BMSCs is also altered, and FD tissue is characterized by abundant osteoclast-like cells that may be essential for lesion expansion. Animal models show local expression of RANKL in bone lesions, and treatment with the RANKL neutralizing antibody denosumab decreased lesion expansion rate in a patient with aggressive FD. However, the role of RANKL/osteoprotegerin (OPG) in FD pathophysiology is not yet understood. We measured serum levels of RANKL, OPG, and inactive RANKL-OPG complexes in FD patients of known disease burden and in healthy volunteers (HVs). RANK, RANKL, and Ki67 immunohistochemistry were assessed in FD tissue. Cultured FD and HV BMSCs were stimulated with prostaglandin E2 (PGE2 ) and 1,25 vitamin D3 to increase RANKL expression, and media levels of RANKL and OPG were measured. Osteoclastogenic induction by FD or HV BMSCs was assessed in co-cultures with HV peripheral monocytes. FD patients showed a 16-fold increase in serum RANKL compared to HVs. OPG was moderately increased (24%), although RANKL/OPG ratio was 12-fold higher in FD patients than in HVs. These measurements were positively correlated with the skeletal burden score (SBS), a validated marker of overall FD burden. No differences in serum inactive RANKL-OPG complexes were observed. In FD tissue, RANKL+ and Ki67+ fibroblastic cells were observed near RANK+ osteoclasts. High levels of RANKL were released by FD BMSCs cultures, but were undetectable in HV cultures. FD BMSC released less OPG than HV BMSCs. FD, but not HV BMSCs, induced osteoclastogenesis in monocyte co-cultures, which was prevented by denosumab addition. These data are consistent with the role of RANKL as a driver in FD-induced osteoclastogenesis. © 2018 American Society for Bone and Mineral Research.
Trial registration: ClinicalTrials.gov NCT00001727.
Keywords: FIBROUS DYSPLASIA; MCCUNE ALBRIGHT SYNDROME; OPG; RANK; RANKL.
© 2018 American Society for Bone and Mineral Research.
Conflict of interest statement
Disclosures
All authors state that they have no conflicts of interest.
Figures
References
-
- Weinstein LS, Shenker A, Gejman PV, Merino MJ, Friedman E, Spiegel AM. Activating mutations of the stimulatory G protein in the McCune-Albright syndrome. N Engl J Med. 1991;325(24): 1688–95. - PubMed
-
- Riminucci M, Saggio I, Robey PG, Bianco P. Fibrous dysplasia as a stem cell disease. J Bone Miner Res. 2006;21 Suppl 2:P125–31. - PubMed
-
- Riminucci M, Liu B, Corsi A, et al. The histopathology of fibrous dysplasia of bone in patients with activating mutations of the Gs alpha gene: site-specific patterns and recurrent histological hall-marks. J Pathol. 1999;187(2):249–58. - PubMed
-
- Collins MT, Kushner H, Reynolds JC, et al. An instrument to measure skeletal burden and predict functional outcome in fibrous dysplasia of bone. J Bone Miner Res. 2005;20(2):219–26. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
