

Intra-articular treatment options for knee osteoarthritis
- PMID: 30498258
- PMCID: PMC6390843
- DOI: 10.1038/s41584-018-0123-4
Intra-articular treatment options for knee osteoarthritis
Abstract
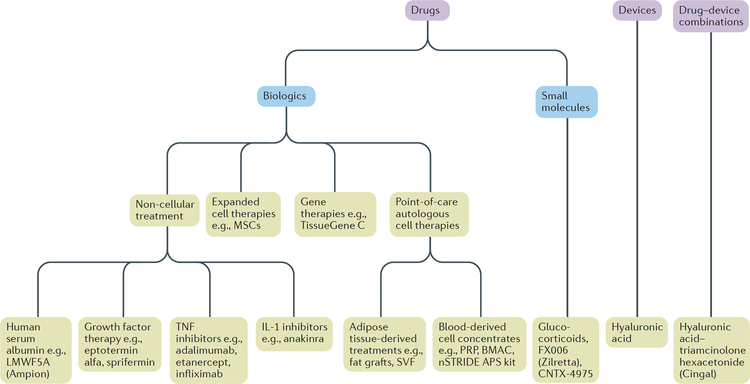
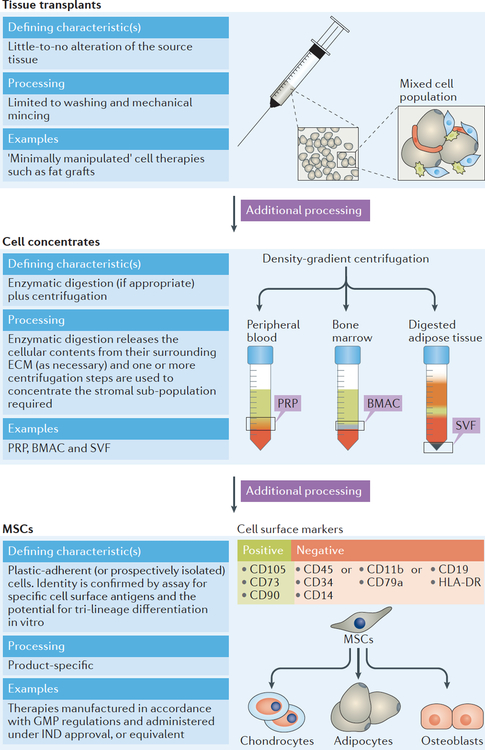
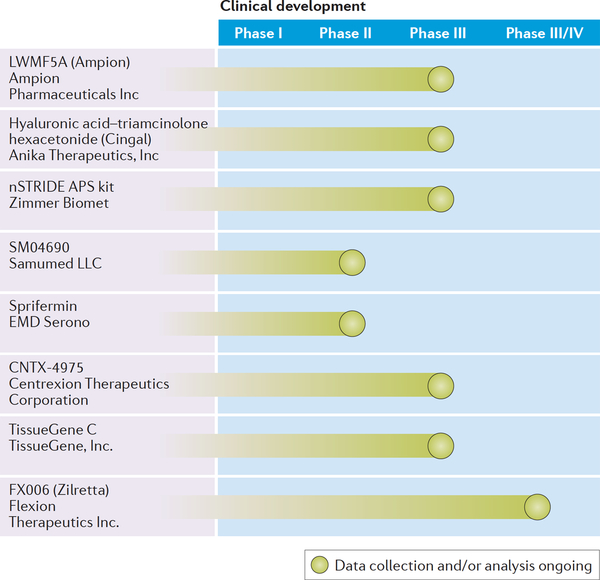
Intra-articular drug delivery has a number of advantages over systemic administration; however, for the past 20 years, intra-articular treatment options for the management of knee osteoarthritis (OA) have been limited to analgesics, glucocorticoids, hyaluronic acid (HA) and a small number of unproven alternative therapies. Although HA and glucocorticoids can provide clinically meaningful benefits to an appreciable number of patients, emerging evidence indicates that the apparent effectiveness of these treatments is largely a result of other factors, including the placebo effect. Biologic drugs that target inflammatory processes are used to manage rheumatoid arthritis, but have not translated well into use in OA. A lack of high-level evidence and methodological limitations hinder our understanding of so-called 'stem' cell therapies and, although the off-label administration of intra-articular cell therapies (such as platelet-rich plasma and bone marrow aspirate concentrate) is common, high-quality clinical data are needed before these treatments can be recommended. A number of promising intra-articular treatments are currently in clinical development in the United States, including small-molecule and biologic therapies, devices and gene therapies. Although the prospect of new, non-surgical treatments for OA is exciting, the benefits of new treatments must be carefully weighed against their costs and potential risks.
Conflict of interest statement
Competing interests
I.A.J., R.T., M.L.W. and N.H. declare no competing interests. C.T.V.Jr. declares that he holds shares in CarthroniX Inc. and in Parcus Medical.
Figures
References
-
- Sinusas K Osteoarthritis: diagnosis and treatment. Am Fam Physician (2012). - PubMed
-
- Aigner T, Söder S, Gebhard PM, McAlinden A & Haag J Mechanisms of disease: role of chondrocytes in the pathogenesis of osteoarthritis--structure, chaos and senescence. Nature clinical practice. Rheumatology 3, 391–399 (2007). - PubMed
-
- Chevalier X, Eymard F & Richette P Biologic agents in osteoarthritis: hopes and disappointments. Nature Reviews Rheumatology 9, 400–410 (2013). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
