

Prolonged action potential duration and dynamic transmural action potential duration heterogeneity underlie vulnerability to ventricular tachycardia in patients undergoing ventricular tachycardia ablation
- PMID: 30500897
- PMCID: PMC6452309
- DOI: 10.1093/europace/euy260
Prolonged action potential duration and dynamic transmural action potential duration heterogeneity underlie vulnerability to ventricular tachycardia in patients undergoing ventricular tachycardia ablation
Abstract
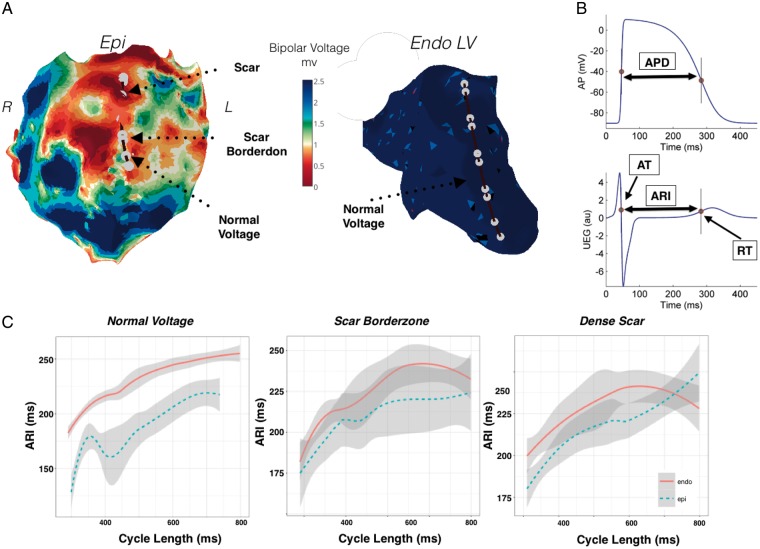
Aims: Differences of action potential duration (APD) in regions of myocardial scar and their borderzones are poorly defined in the intact human heart. Heterogeneities in APD may play an important role in the generation of ventricular tachycardia (VT) by creating regions of functional block. We aimed to investigate the transmural and planar differences of APD in patients admitted for VT ablation.
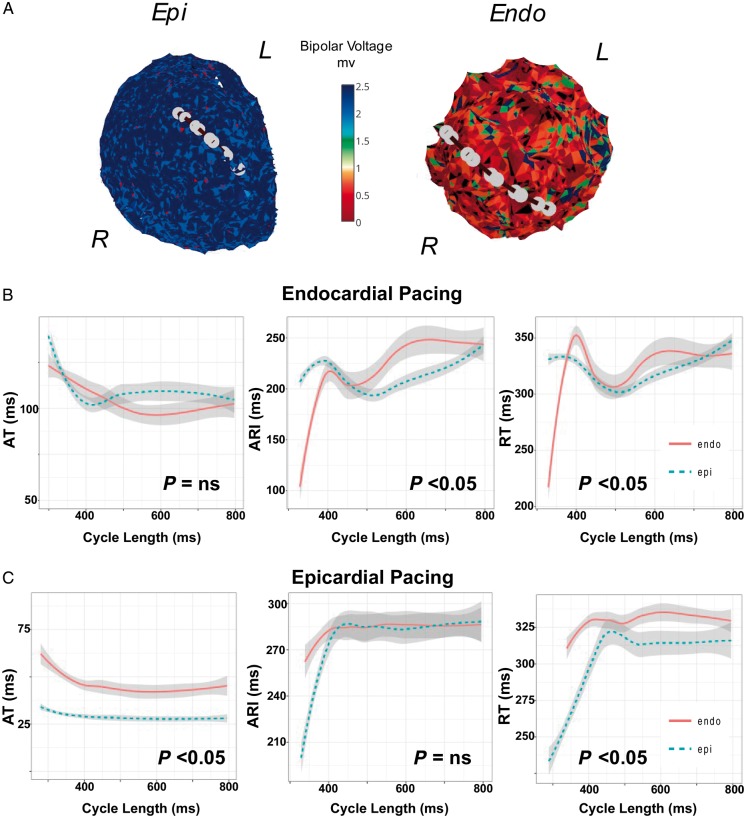
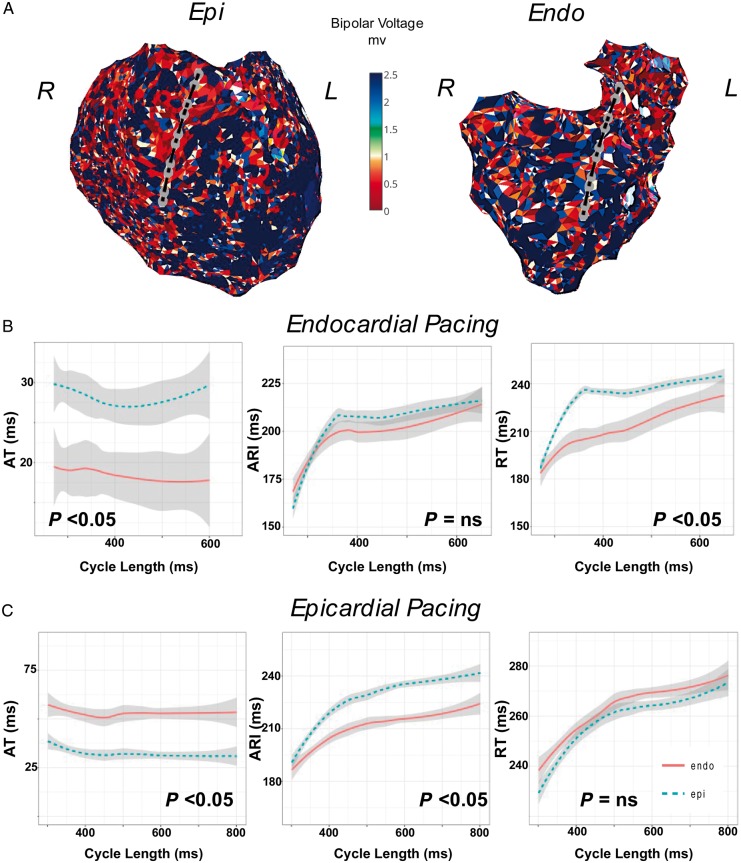
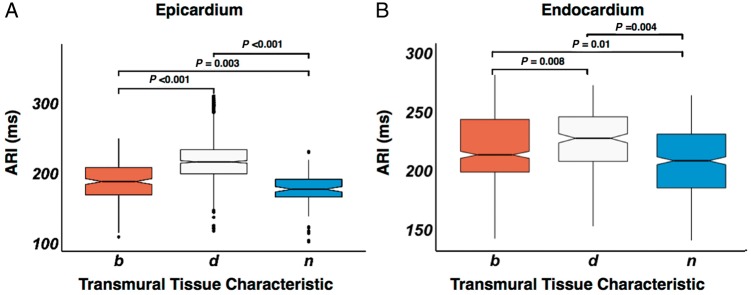
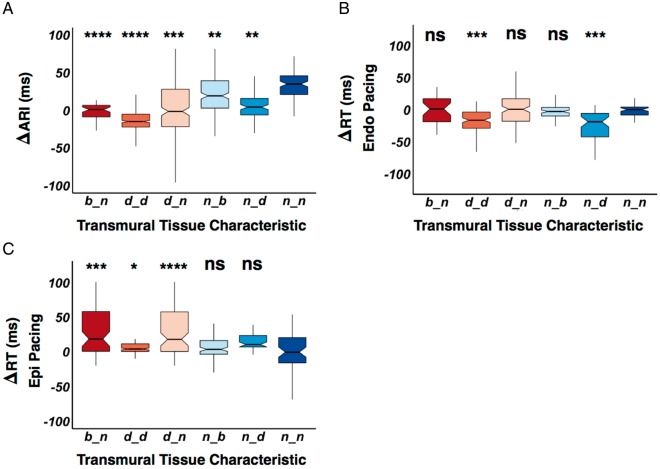
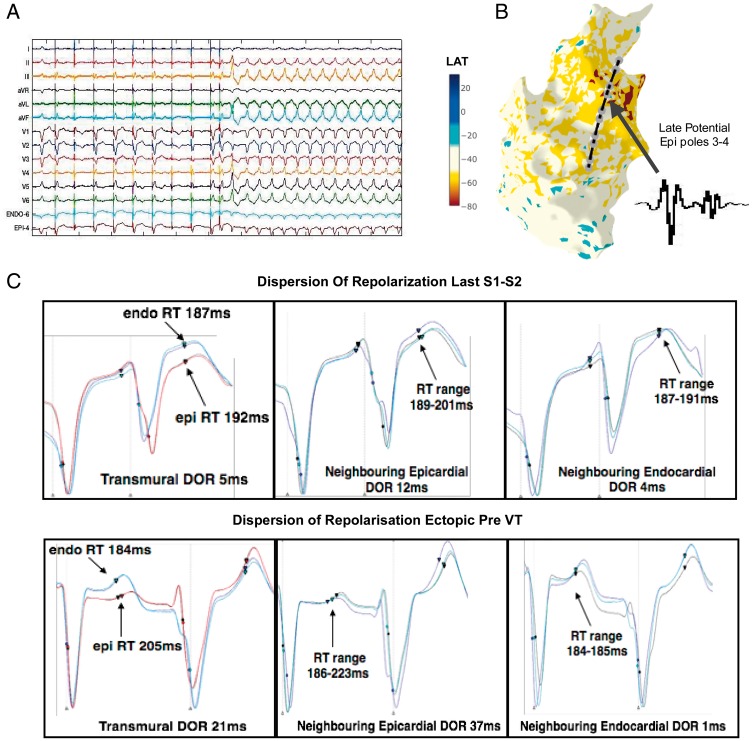
Methods and results: Six patients (median age 53 years, five male); (median ejection fraction 35%), were studied. Endocardial (Endo) and epicardial (Epi) 3D electroanatomic mapping was performed. A bipolar voltage of <0.5 mV was defined as dense scar, 0.5-1.5 mV as scar borderzone, and >1.5 mV as normal. Decapolar catheters were positioned transmurally across the scar borderzone to assess differences of APD and repolarization time (RT) during restitution pacing from Endo and Epi. Epi APD was 173 ms in normal tissue vs. 187 ms at scar borderzone and 210 ms in dense scar (P < 0.001). Endocardial APD was 210 ms in normal tissue vs. 222 ms in the scar borderzone and 238 ms in dense scar (P < 0.01). This resulted in significant transmural RT dispersion (ΔRT 22 ms across dense transmural scar vs. 5 ms in normal transmural tissue, P < 0.001), dependent on the scar characteristics in the Endo and Epi, and the pacing site.
Conclusion: Areas of myocardial scar have prolonged APD compared with normal tissue. Heterogeneity of regional transmural and planar APD result in localized dispersion of repolarization, which may play an important role in initiating VT.
Keywords: Action potential duration; Dispersion of repolarization; Transmural dispersion of repolarization; Ventricular tachycardia.
© The Author(s) 2018. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Similar articles
-
Layered activation of epicardial scar in arrhythmogenic right ventricular dysplasia: possible substrate for confined epicardial circuits.Circ Arrhythm Electrophysiol. 2012 Aug 1;5(4):796-803. doi: 10.1161/CIRCEP.111.967935. Epub 2012 May 25. Circ Arrhythm Electrophysiol. 2012. PMID: 22634228
-
Ventricular Tachycardia in the Setting of Chagasic Cardiomyopathy: Use of Voltage Mapping to Characterize Endoepicardial Nonischemic Scar Distribution.Circ Arrhythm Electrophysiol. 2017 Nov;10(11):e004950. doi: 10.1161/CIRCEP.116.004950. Circ Arrhythm Electrophysiol. 2017. PMID: 29133379
-
Utility of ripple mapping for identification of slow conduction channels during ventricular tachycardia ablation in the setting of arrhythmogenic right ventricular cardiomyopathy.J Cardiovasc Electrophysiol. 2019 Mar;30(3):366-373. doi: 10.1111/jce.13819. Epub 2019 Jan 6. J Cardiovasc Electrophysiol. 2019. PMID: 30575168 Free PMC article.
-
Endo-epicardial vs endocardial-only catheter ablation of ventricular tachycardia: A meta-analysis.J Cardiovasc Electrophysiol. 2019 Sep;30(9):1537-1548. doi: 10.1111/jce.14013. Epub 2019 Jul 2. J Cardiovasc Electrophysiol. 2019. PMID: 31172632
-
Myocardial voltage ratio in arrhythmogenic right ventricular dysplasia/cardiomyopathy.Herzschrittmacherther Elektrophysiol. 2017 Jun;28(2):219-224. doi: 10.1007/s00399-017-0508-0. Epub 2017 May 23. Herzschrittmacherther Elektrophysiol. 2017. PMID: 28536891 Review. English.
Cited by
-
Multicenter Study of Dynamic High-Density Functional Substrate Mapping Improves Identification of Substrate Targets for Ischemic Ventricular Tachycardia Ablation.JACC Clin Electrophysiol. 2020 Dec;6(14):1783-1793. doi: 10.1016/j.jacep.2020.06.037. Epub 2020 Sep 16. JACC Clin Electrophysiol. 2020. PMID: 33357574 Free PMC article.
-
Effect of scar and pacing location on repolarization in a porcine myocardial infarction model.Heart Rhythm O2. 2022 Jan 26;3(2):186-195. doi: 10.1016/j.hroo.2022.01.008. eCollection 2022 Apr. Heart Rhythm O2. 2022. PMID: 35496454 Free PMC article.
-
Epicardial ablation of ventricular tachycardia in ischemic cardiomyopathy: A review and local experience.Indian Pacing Electrophysiol J. 2024 Mar-Apr;24(2):84-93. doi: 10.1016/j.ipej.2024.02.002. Epub 2024 Feb 8. Indian Pacing Electrophysiol J. 2024. PMID: 38340957 Free PMC article. Review.
-
Conduction Velocity Dispersion Predicts Postinfarct Ventricular Tachycardia Circuit Sites and Associates With Lipomatous Metaplasia.JACC Clin Electrophysiol. 2023 Aug;9(8 Pt 2):1464-1474. doi: 10.1016/j.jacep.2023.05.013. Epub 2023 May 18. JACC Clin Electrophysiol. 2023. PMID: 37294264 Free PMC article.
-
Complex repolarization dynamics in ex vivo human ventricles are independent of the restitution properties.Europace. 2023 Dec 6;25(12):euad350. doi: 10.1093/europace/euad350. Europace. 2023. PMID: 38006390 Free PMC article.
References
-
- Marchlinski FE, Callans DJ, Gottlieb CD, Zado E.. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation 2000;101:1288–96. - PubMed
-
- Reddy VY, Neuzil P, Taborsky M, Ruskin JN.. Short-term results of substrate mapping and radiofrequency ablation of ischemic ventricular tachycardia using a saline-irrigated catheter. J Am Coll Cardiol 2003;41:2228–36. - PubMed
-
- Delacretaz E, Stevenson WG.. Catheter ablation of ventricular tachycardia in patients with coronary heart disease: part I: mapping. Pacing Clin Electrophysiol 2001;24:1261–77. - PubMed
-
- Taggart P. Transmural repolarisation in the left ventricle in humans during normoxia and ischaemia. Cardiovasc Res 2001;50:454–62. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
