

Mortality and morbidity following exercise-based renal rehabilitation in patients with chronic kidney disease: the effect of programme completion and change in exercise capacity
- PMID: 30500926
- PMCID: PMC6452180
- DOI: 10.1093/ndt/gfy351
Mortality and morbidity following exercise-based renal rehabilitation in patients with chronic kidney disease: the effect of programme completion and change in exercise capacity
Erratum in
-
Erratum.Nephrol Dial Transplant. 2020 Aug 1;35(8):1452. doi: 10.1093/ndt/gfz032. Nephrol Dial Transplant. 2020. PMID: 30770707 Free PMC article. No abstract available.
Abstract
Background: Twelve weeks of renal rehabilitation (RR) have been shown to improve exercise capacity in patients with chronic kidney disease (CKD); however, survival following RR has not been examined.
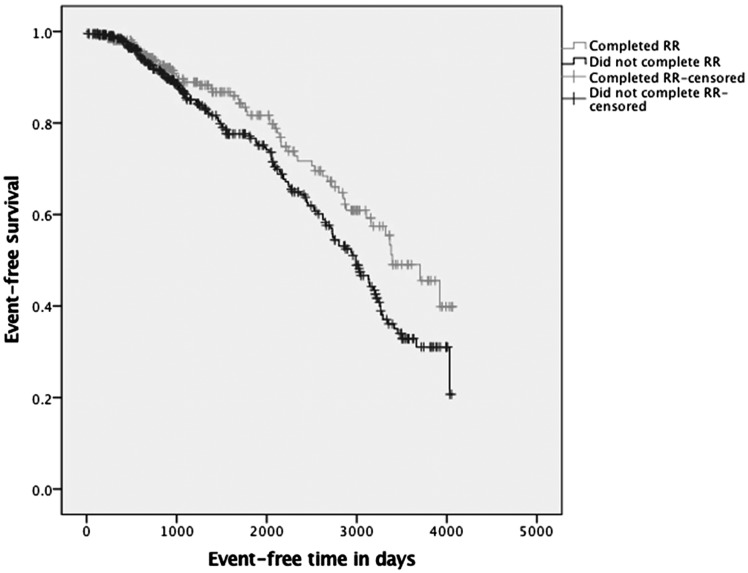
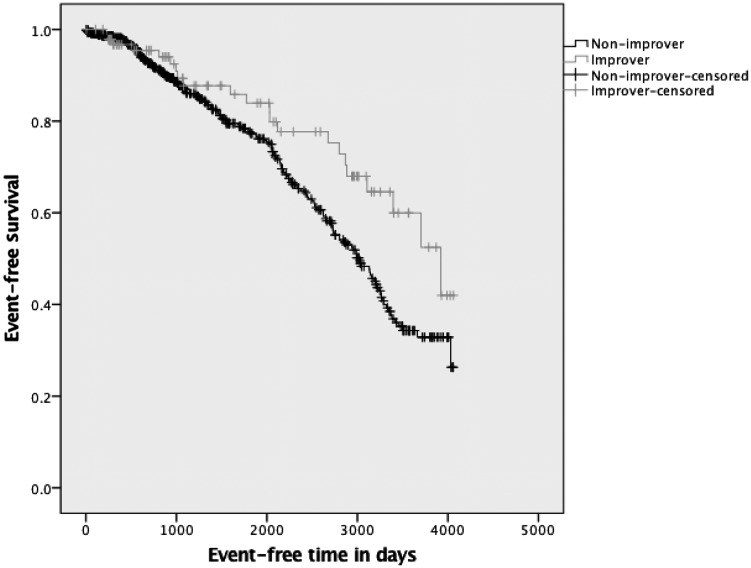
Methods: This study included a retrospective longitudinal analysis of clinical service outcomes. Programme completion and improvement in exercise capacity, characterised as change in incremental shuttle walk test (ISWT), were analysed with Kaplan-Meier survival analyses to predict risk of a combined event including death, cerebrovascular accident, myocardial infarction and hospitalisation for heart failure in a cohort of patients with CKD. Time to combined event was examined with Kaplan-Meier plots and log rank test between 'completers' (attended >50% planned sessions) and 'non-completers'. In completers, time to combined event was examined between 'improvers' (≥50 m increase ISWT) and 'non-improvers' (<50 m increase). Differences in time to combined event were investigated with Cox proportional hazards models (adjusted for baseline kidney function, body mass index, diabetes, age, gender, ethnicity, baseline ISWT and smoking status).
Results: In all, 757 patients (male 54%) (242 haemodialysis patients, 221 kidney transplant recipients, 43 peritoneal dialysis patients, 251 non-dialysis CKD patients) were referred for RR between 2005 and 2017. There were 193 events (136 deaths) during the follow-up period (median 34 months). A total of 43% of referrals were classified as 'completers', and time to event was significantly greater when compared with 'non-completers' (P = 0.009). Responding to RR was associated with improved event-free survival time (P = 0.02) with Kaplan-Meier analyses and log rank test. On multivariate analysis, completing RR contributed significantly to the minimal explanatory model relating clinical variables to the combined event (overall χ2 = 38.0, P < 0.001). 'Non-completers' of RR had a 1.6-fold [hazard ratio = 1.6; 95% confidence interval (CI) 1.00-2.58] greater risk of a combined event (P = 0.048). Change in ISWT of >50 m contributed significantly to the minimal explanatory model relating clinical variables to mortality and morbidity (overall χ2 = 54.0, P < 0.001). 'Improvers' had a 40% (hazard ratio = 0.6; 95% CI 0.36-0.98) independent lower risk of a combined event (P = 0.041).
Conclusions: There is an association between completion of an RR programme, and also RR success, and a lower risk of a combined event in this observational study. RR interventions to improve exercise capacity in patients with CKD may reduce risk of morbidity and mortality, and a pragmatic randomised controlled intervention trial is warranted.
Keywords: chronic kidney disease; morbidity; mortality; rehabilitation; survival.
© The Author(s) 2018. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
Comment in
-
Time to rehabilitate the idea of exercise for patients with chronic kidney disease?Nephrol Dial Transplant. 2019 Apr 1;34(4):551-554. doi: 10.1093/ndt/gfz030. Nephrol Dial Transplant. 2019. PMID: 30824930 Free PMC article. No abstract available.
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC. et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003; 108: 2154–2169 - PubMed
-
- Greenwood SA, Lindup H, Taylor K. et al. Evaluation of a pragmatic exercise rehabilitation programme in chronic kidney disease. Nephrol Dial Transplant 2012; 27: iii126. - PubMed
-
- Greenwood SA, Koufaki P, Mercer TH. et al. Effect of exercise training on estimated GFR, vascular health, and cardiorespiratory fitness in patients with CKD: a pilot randomized controlled trial. Am J Kidney Dis 2015; 65: 425–434 - PubMed
-
- Greenwood SA, Koufaki P, Mercer TH. et al. Aerobic or resistance training and pulse wave velocity in kidney transplant recipients: a 12-week pilot randomized controlled trial (the Exercise in Renal Transplant [ExeRT] Trial). Am J Kidney Dis 2015; 66: 689–698 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
