

A randomized, double-blind, phase III trial of personalized peptide vaccination for recurrent glioblastoma
- PMID: 30500939
- PMCID: PMC6380422
- DOI: 10.1093/neuonc/noy200
A randomized, double-blind, phase III trial of personalized peptide vaccination for recurrent glioblastoma
Abstract
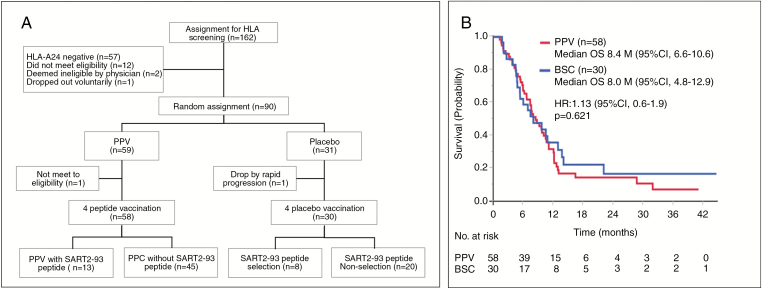
Background: We conducted a phase III trial of personalized peptide vaccination (PPV) for human leukocyte antigen (HLA)-A24+ recurrent glioblastoma to develop a new treatment modality.
Methods: We randomly assigned 88 recurrent glioblastoma patients to receive PPV (n = 58) or the placebo (n = 30) at a 2-to-1 ratio. Four of 12 warehouse peptides selected based on preexisting peptide-specific immunoglobulin G levels or the corresponding placebos were injected 1×/week for 12 weeks.
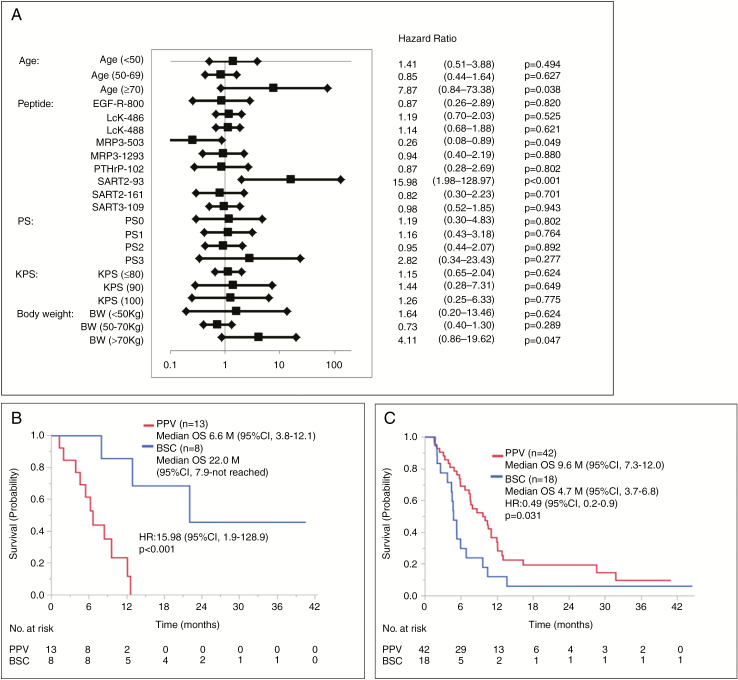
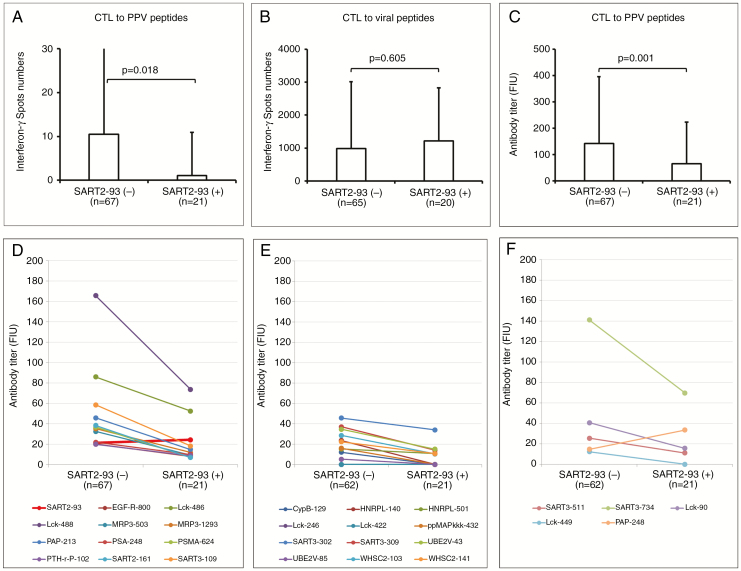
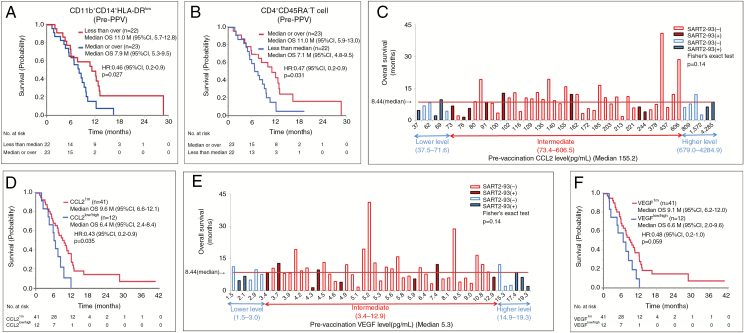
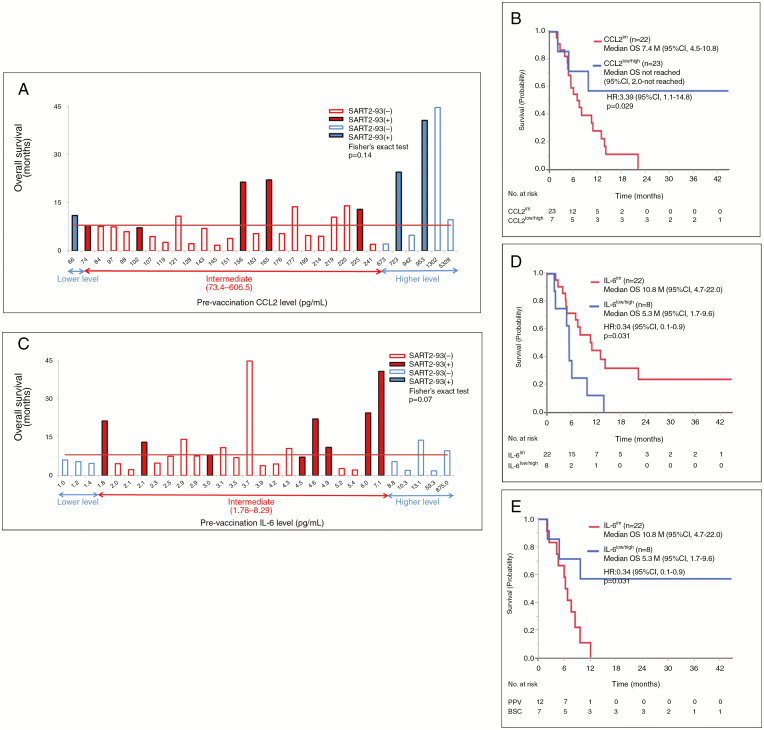
Results: Our trial met neither the primary (overall survival [OS]) nor secondary endpoints. Unfavorable factors for OS of 58 PPV patients compared with 30 placebo patients were SART2-93 peptide selection (n = 13 vs 8, hazard ratio [HR]: 15.9), ≥70 years old (4 vs 4, 7.87), >70 kg body weight (10 vs 7, 4.11), and performance status (PS)3 (8 vs 2, 2.82), respectively. Consequently, the median OS for PPV patients without SART2-93 selection plus one of these 3 favorable factors (<70 y old, ≤70 kg, or PS0-2) was significantly longer than that for the corresponding placebo patients (HR: 0.49, 0.44, and 0.51), respectively. Preexisting immunity against both all 12 warehouse peptides besides SART2-93 and the other cytotoxic T lymphocyte epitope peptides was significantly depressed in the patients with SART2-93 selection (n = 21) compared with that of the patients without SART2-93 selection (n = 67). Biomarkers correlative for favorable OS of the PPV patients were a lower percentage of CD11b+CD14+HLA-DRlow immunosuppressive monocytes and a higher percentage of CD4+CD45RA- activated T cells, the intermediate levels of chemokine C-C ligand 2 (CCL2), vascular endothelial growth factor, interleukin (IL)-6, IL-17, or haptoglobin, respectively.
Conclusion: This phase III trial met neither the primary nor secondary endpoints.
Keywords: biomarker for overall survival; personalized peptide vaccine; phase III trial; pre-existing immunity; recurrent glioblastoma.
© The Author(s) 2018. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Bespoke immunotherapy: how close are we?Neuro Oncol. 2019 Feb 19;21(3):289-290. doi: 10.1093/neuonc/noz017. Neuro Oncol. 2019. PMID: 31222359 Free PMC article. No abstract available.
References
-
- Friedman HS, Prados MD, Wen PY, et al. . Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol. 2009;27(28):4733–4740. - PubMed
-
- Taal W, Oosterkamp HM, Walenkamp AM, et al. . Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): a randomised controlled phase 2 trial. Lancet Oncol. 2014;15(9):943–953. - PubMed
-
- Cloughesy T, Finocchiaro G, Belda-Iniesta C, et al. . Randomized, double-blind, placebo-controlled, multicenter phase II study of onartuzumab plus bevacizumab versus placebo plus bevacizumab in patients with recurrent glioblastoma: efficacy, safety, and hepatocyte growth factor and O6-methylguanine-DNA methyltransferase biomarker analyses. J Clin Oncol. 2017;35(3):343–351. - PubMed
-
- Purcell AW, McCluskey J, Rossjohn J. More than one reason to rethink the use of peptides in vaccine design. Nat Rev Drug Discov. 2007;6(5):404–414. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
