

Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL
- PMID: 30501481
- PMCID: PMC6325637
- DOI: 10.1056/NEJMoa1812836
Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL
Abstract
Background: Ibrutinib has been approved by the Food and Drug Administration for the treatment of patients with untreated chronic lymphocytic leukemia (CLL) since 2016 but has not been compared with chemoimmunotherapy. We conducted a phase 3 trial to evaluate the efficacy of ibrutinib, either alone or in combination with rituximab, relative to chemoimmunotherapy.
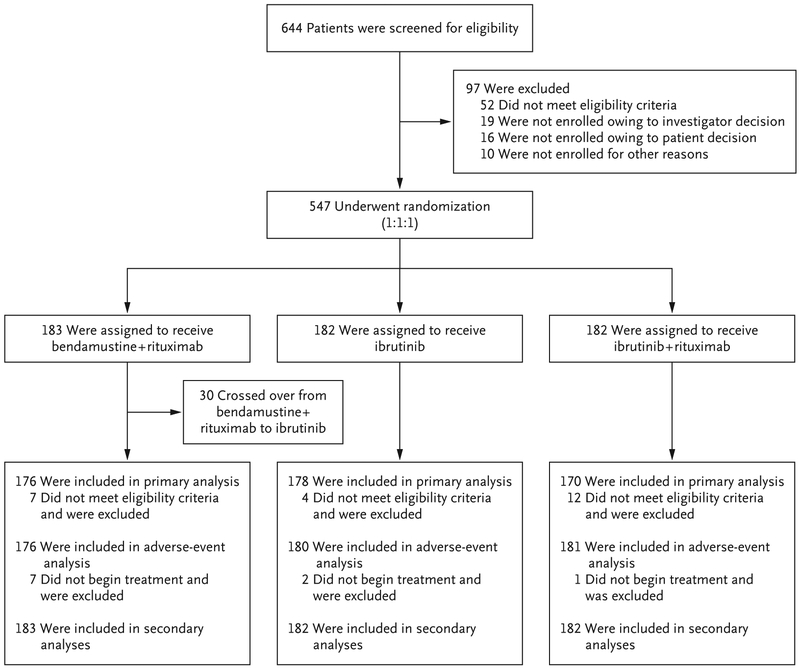
Methods: Patients 65 years of age or older who had untreated CLL were randomly assigned to receive bendamustine plus rituximab, ibrutinib, or ibrutinib plus rituximab. The primary end point was progression-free survival. The Alliance Data and Safety Monitoring Board made the decision to release the data after the protocol-specified efficacy threshold had been met.
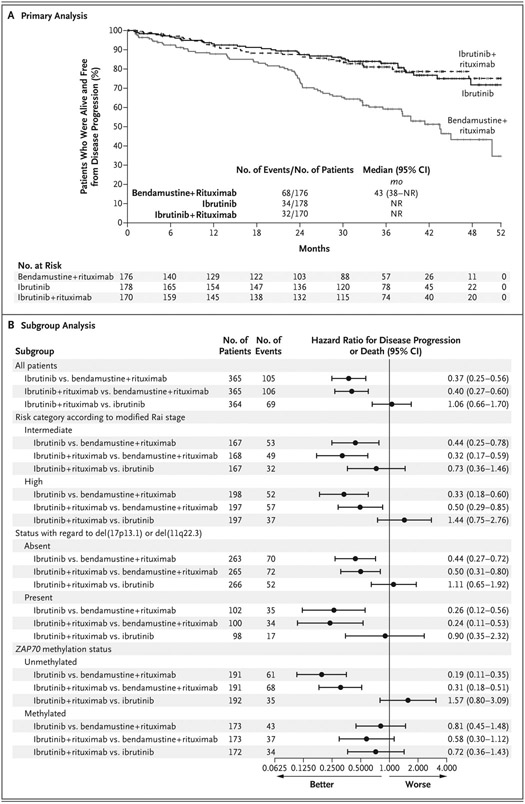
Results: A total of 183 patients were assigned to receive bendamustine plus rituximab, 182 to receive ibrutinib, and 182 to receive ibrutinib plus rituximab. Median progression-free survival was reached only with bendamustine plus rituximab. The estimated percentage of patients with progression-free survival at 2 years was 74% with bendamustine plus rituximab and was higher with ibrutinib alone (87%; hazard ratio for disease progression or death, 0.39; 95% confidence interval [CI], 0.26 to 0.58; P<0.001) and with ibrutinib plus rituximab (88%; hazard ratio, 0.38; 95% CI, 0.25 to 0.59; P<0.001). There was no significant difference between the ibrutinib-plus-rituximab group and the ibrutinib group with regard to progression-free survival (hazard ratio, 1.00; 95% CI, 0.62 to 1.62; P=0.49). With a median follow-up of 38 months, there was no significant difference among the three treatment groups with regard to overall survival. The rate of grade 3, 4, or 5 hematologic adverse events was higher with bendamustine plus rituximab (61%) than with ibrutinib or ibrutinib plus rituximab (41% and 39%, respectively), whereas the rate of grade 3, 4, or 5 nonhematologic adverse events was lower with bendamustine plus rituximab (63%) than with the ibrutinib-containing regimens (74% with each regimen).
Conclusions: Among older patients with untreated CLL, treatment with ibrutinib was superior to treatment with bendamustine plus rituximab with regard to progression-free survival. There was no significant difference between ibrutinib and ibrutinib plus rituximab with regard to progression-free survival. (Funded by the National Cancer Institute and Pharmacyclics; ClinicalTrials.gov number, NCT01886872 .).
Figures
Comment in
-
Ibrutinib Regimens in Older Patients with Untreated CLL.N Engl J Med. 2019 Apr 25;380(17):1679. doi: 10.1056/NEJMc1901284. N Engl J Med. 2019. PMID: 31018078 No abstract available.
-
Ibrutinib Regimens in Older Patients with Untreated CLL.N Engl J Med. 2019 Apr 25;380(17):1679. doi: 10.1056/NEJMc1901284. N Engl J Med. 2019. PMID: 31018079 No abstract available.
-
Ibrutinib Regimens in Older Patients with Untreated CLL.N Engl J Med. 2019 Apr 25;380(17):1679-1681. doi: 10.1056/NEJMc1901284. N Engl J Med. 2019. PMID: 31018080 No abstract available.
References
-
- Goede V, Fischer K, Busch R, et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med 2014;370:1101–10. - PubMed
-
- Eichhorst B, Fink AM, Bahlo J, et al. First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol 2016; 17:928–42. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R01 CA197870/CA/NCI NIH HHS/United States
- K23 CA178183/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- UG1 CA232760/CA/NCI NIH HHS/United States
- R01 CA183444/CA/NCI NIH HHS/United States
- UG1 CA189823/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- P30 CA016058/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- R35 CA197734/CA/NCI NIH HHS/United States
- U10 CA180836/CA/NCI NIH HHS/United States
- UG1 CA189858/CA/NCI NIH HHS/United States
- U10 CA180857/CA/NCI NIH HHS/United States
- U10 CA180850/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- P30 CA033572/CA/NCI NIH HHS/United States
- U10 CA180833/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous